Author
Dr Chary Duraikannu
Consultant Radiologist, Ninewells Hospital and Medical School, NHS Tayside, Dundee, UK.
Case history
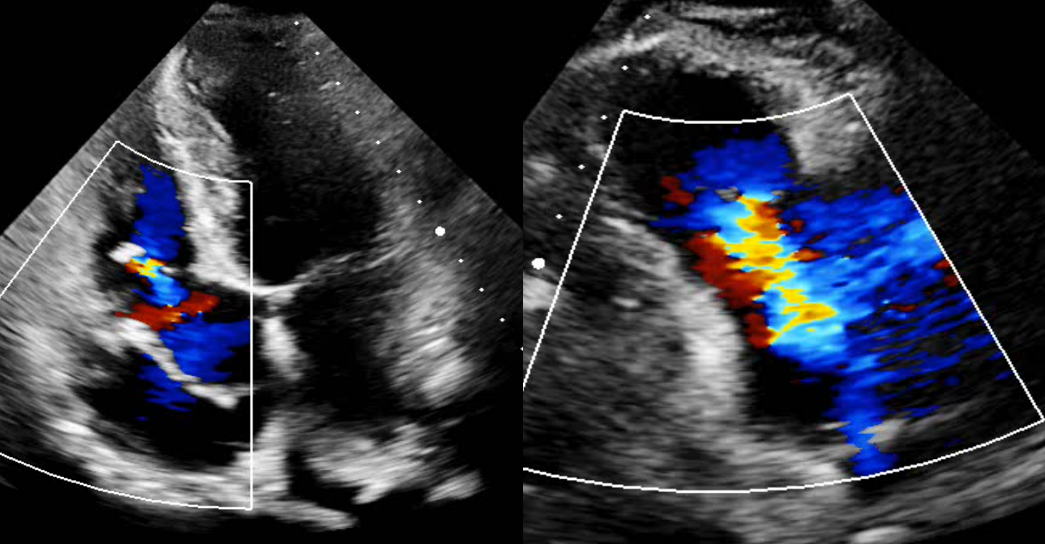
A 54-year-old male with a long-standing murmur presents for evaluation. A prior transesophageal echocardiogram revealed no septal defects but noted a slightly abnormal appearance of the mitral valve. The patient recently experienced a collapse and has a loop recorder in situ. Previous ECG findings included intraventricular conduction delay, right bundle branch block, and left axis deviation of the QRS complex, with a normal PR interval.
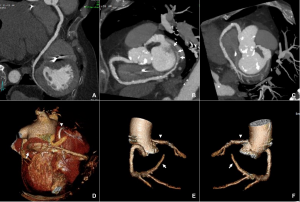
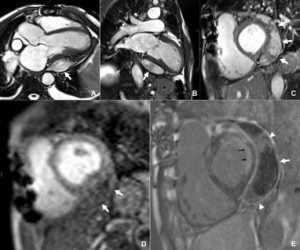
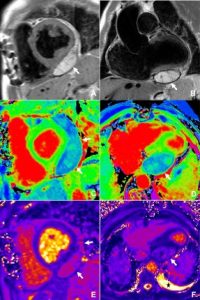
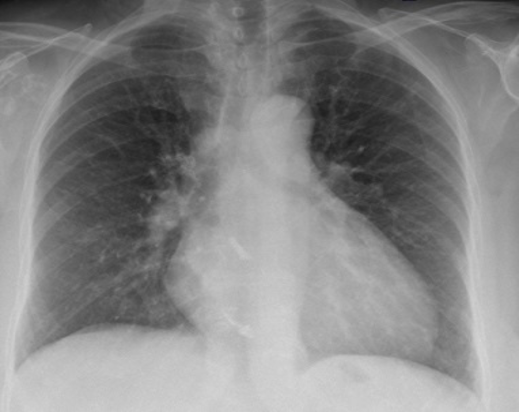
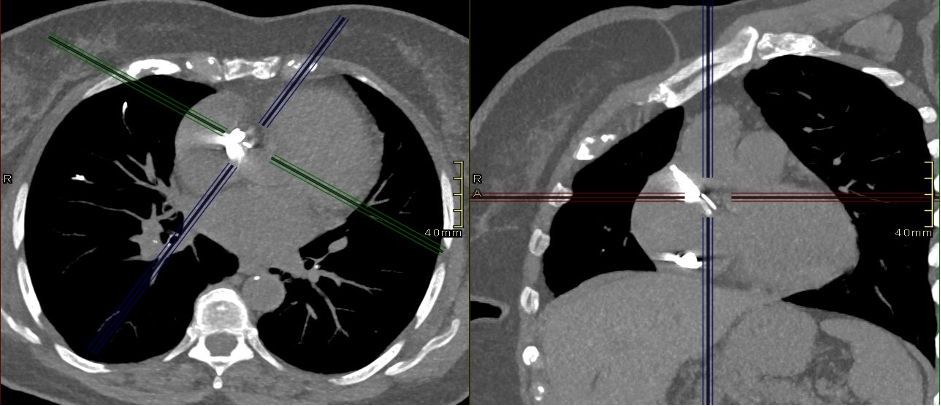
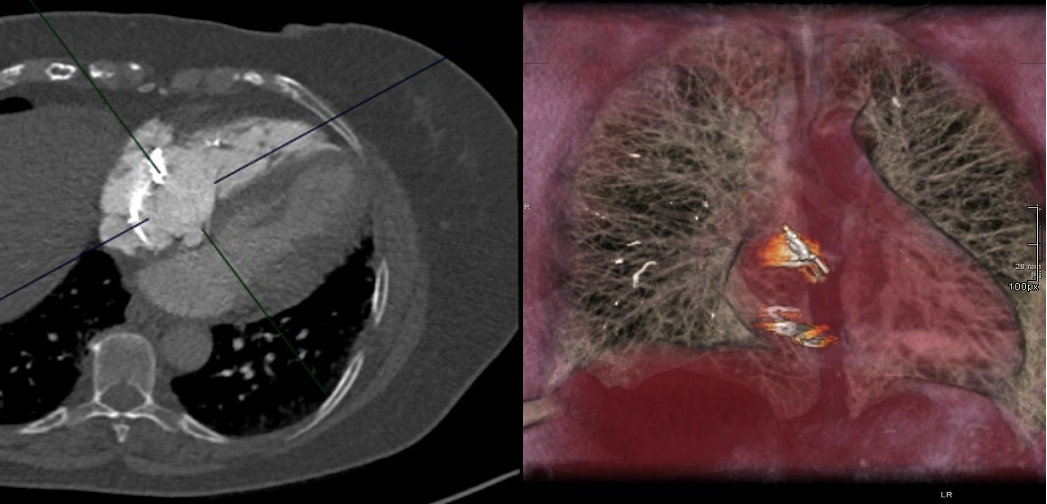
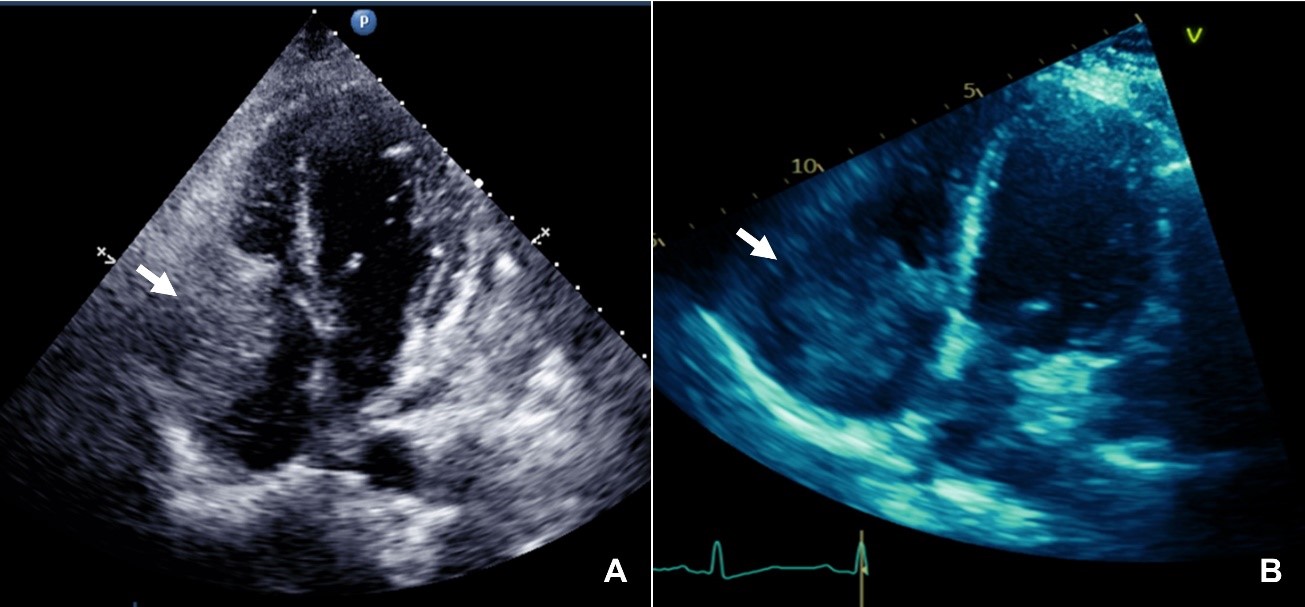
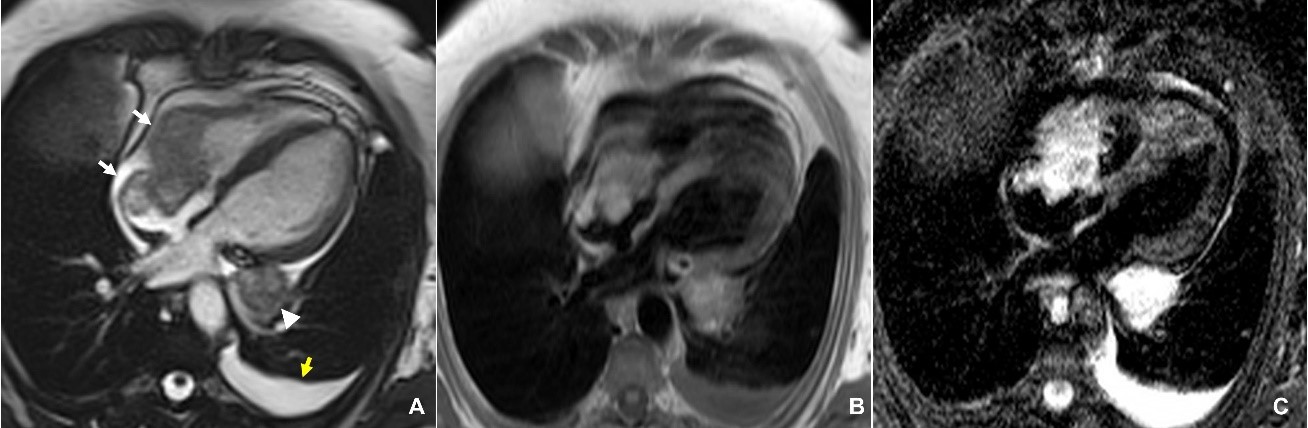
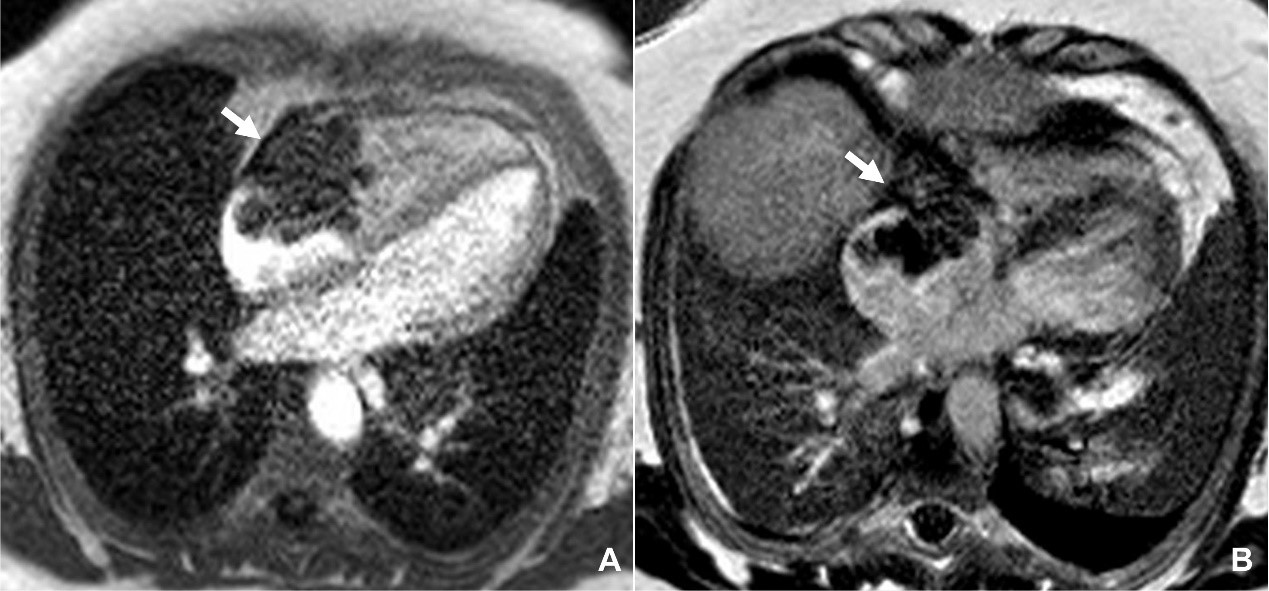
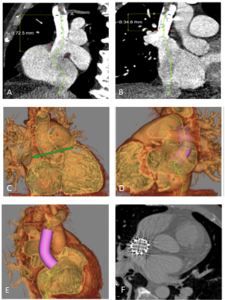
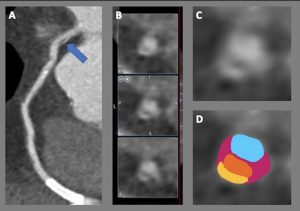
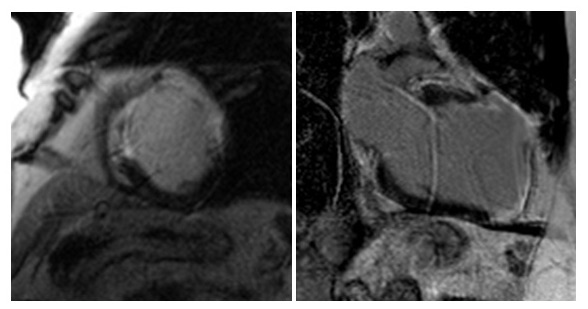
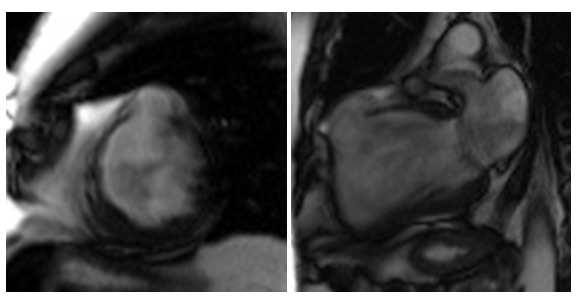
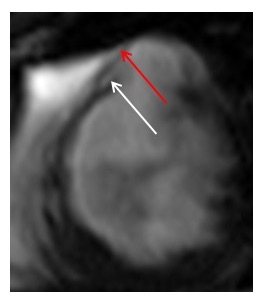
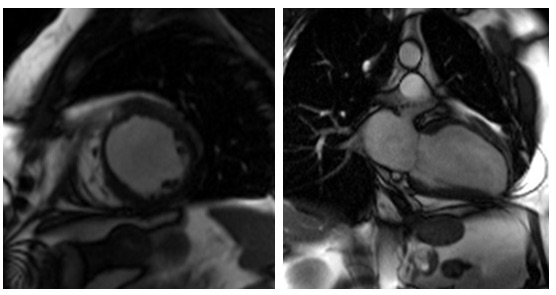
CT and MRI shows complete leftward deviation of heart and midline position of trachea. Interposition of lung tissue noted at aorto-pulmonary window and also discontinuous segment of pericardium in anterior aspect. The heart was otherwise structurally normal, and no intervention was carried out.

Questions
1. Which of the following are imaging features of pericardial agenesis ?
- Excessive levorotation
- Interposition of lung tissue at aortopulmonary window
- Discontinuous segments of the pericardium in anterior aspect
- Midline position of the trachea
- All of the above
2. Which statement is false ?
- Normal pericardium is 1-2mm thick
- Pericardium is easily identified along the posterior wall of left ventricle
- Pericardial agenesis can be misdiagnosed due to non-specific symptoms
- ECG changes include right axis deviation with incomplete RBBB
- None of the above
3. Which of the statement is true regarding congenital absence of the pericardium?
- Larger defects are typically symptomatic.
- Right sided pericardial defects are common than left sided defects.
- Risk of herniation of the left atrial appendage in smaller defects.
- Majority of patients require surgical intervention.
- Cuvier duct regression is not related to pericardial agenesis.
(Answers:e,b,c)
Discussion
Congenital absence of the pericardium is an exceedingly rare anomaly categorized as partial or total defects. Most prevalent are complete left sided defects (70%) followed by complete right sided (17%), complete bilateral (9%) and partial right or left sided (3-4%) [1,2]. Associated congenital anomalies include atrial septal defects, patent ductus arteriosus, mitral valve disease, tetralogy of fallot, and sinus venosus defects with partial anomalous pulmonary venous drainage [3].
In the 5th week of embryonic development pleuropericardial membranes fuse to form pericardium. Failure of this process occurs due to premature regression of ducts of cuvier results in pericardial agenesis [1].
Complete agenesis of pericardium is usually asymptomatic or present with non-specific symptoms. These are mostly incidental during cross sectional imaging performed for other reasons or cardiothoracic surgery [4,5]. However, smaller defects can present with chest pain and dyspnoea when lying on one side and pose risks such as herniation of the left atrial appendage or compression of the left coronary artery [4,6].
Normal pericardium is 1-2 mm in thickness and is usually seen in CT and MRI because of surrounding adipose tissue. Its visualization can be difficult posterior and lateral to left ventricle due to paucity of pericardial fat [7].
Frequently, the electrocardiogram displays bradycardia with right bundle branch block. Additionally, poor R wave progression as well as large P waves may be observed [8].
Diagnosing congenital pericardial defects often relies on indirect signs. Typical findings in cross sectional imaging include excessive levorotation with the left ventricular apex pointing posteriorly, lung interposition at the aorto-pulmonary window and between the base of the heart and the diaphragm, and discontinuous segments of pericardium along the anterior aspect and midline trachea [9,10].
In case of complete bilateral or complete left-sided absence of the pericardium, no treatment is generally indicated [1,11]. Symptomatic patients with partial defects and cardiac chamber herniation should undergo surgery. Treatment options include patch closure of the defect, pericardiectomy, or pericardioplasty [12,13].
Reference:
1.Nasser WK. Congenital diseases of the pericardium. Cardiovasc Clin. 1976;7(3):271-86. PMID: 826317.
2.Klein AL, Abbara S, Agler DA, Appleton CP, Asher CR, Hoit B, Hung J, Garcia MJ, Kronzon I, Oh JK, Rodriguez ER, Schaff HV, Schoenhagen P, Tan CD, White RD. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2013 Sep;26(9):965-1012.e15. doi: 10.1016/j.echo.2013.06.023. PMID: 23998693.
3.BremerichJ,ReddyGP,HigginsCB.Magneticresonanceimageofcardiacstructure. In: Pohost GM, O’Rourke RA, Berman D, Shah PM, eds. Imaging in Cardiovascular Disease. Philadelphia: Lippincott Williams & Wilkins; 2000. p409, 756.
4.,Bernardinello V, Cipriani A, Perazzolo Marra M, Motta R, Barchitta A. Congenital pericardial agenesis in asymptomatic individuals: tips for the diagnosis. Circ Cardiovasc Imaging 2020;13:e010169.
5.Shiikawa M, Nakahashi K, Endo M, Shiono S. [Congenital Defect of the Pericardium Incidentally Found during Surgery for Lung Cancer:Report of a Case]. Kyobu Geka. 2021 Apr;74(4):308-312. Japanese. PMID: 33831892.
6.Robin E, Ganguly S, Fowler MS. Strangulation of the left atrial appendage
through a congenital partial pericardial defect. Chest 1975;67:354–55
7.Yared K, Baggish AL, Picard MH, Hoffmann U, Hung J. Multimodality imaging of pericardial diseases. JACC Cardiovasc Imaging. 2010 Jun;3(6):650-60. doi: 10.1016/j.jcmg.2010.04.009. PMID: 20541720.
8.Abbas AE, Appleton CP, Liu PT, Sweeney JP. Congenital absence of the pericardium: case presentation and review of literature. Int J Cardiol. 2005 Jan;98(1):21-5. doi: 10.1016/j.ijcard.2003.10.021. PMID: 15676161.
9.Shah AB, Kronzon I. Congenital defects of the pericardium: a review. Eur Heart J Cardiovasc Imaging. 2015 Aug;16(8):821-7. doi: 10.1093/ehjci/jev119. Epub 2015 May 23. PMID: 26003149.
10.Iijima Y, Ishikawa M, Iwai S, Yamagata A, Motono N, Yamagishi S, Koizumi K, Uramoto H. Congenital partial pericardial defect discovered incidentally during surgery for lung cancer: a case report and literature review. BMC Surg. 2021 Dec 31;21(1):447. doi: 10.1186/s12893-021-01453-3. PMID: 34972509; PMCID: PMC8720205.
11.TanakaH,OishiY,MizuguchiY,MiyoshiH,IshimotoT,NagaseNetal.Contribution of the pericardium to left ventricular torsion and regional myocardial function in patients with total absence of the left pericardium. J Am Soc Echocardiogr 2008;21: 268 – 74.
12.Gatzoulis MA, Munk MD, Merchant N, Van Arsdell GS, McCrindle BW, Webb GD. Isolated congenital absence of the pericardium: clinical presentation, diagnosis, and management. Ann Thorac Surg. 2000 Apr;69(4):1209-15. doi: 10.1016/s0003-4975(99)01552-0. PMID: 10800821.
13.Van Son JA, Danielson DG, Schaff HV, Mullany CJ, Julsud PR, Breen JF. Congenital partial and complete absence of the pericardium. Mayo Clin Proc 1993;68:743–7.