Case Study: an 8 month old child presenting with ischaemic cardiomyopathy
Matt Muller, Philip Gonsalves Radiology SpRs – Newcastle Hospitals
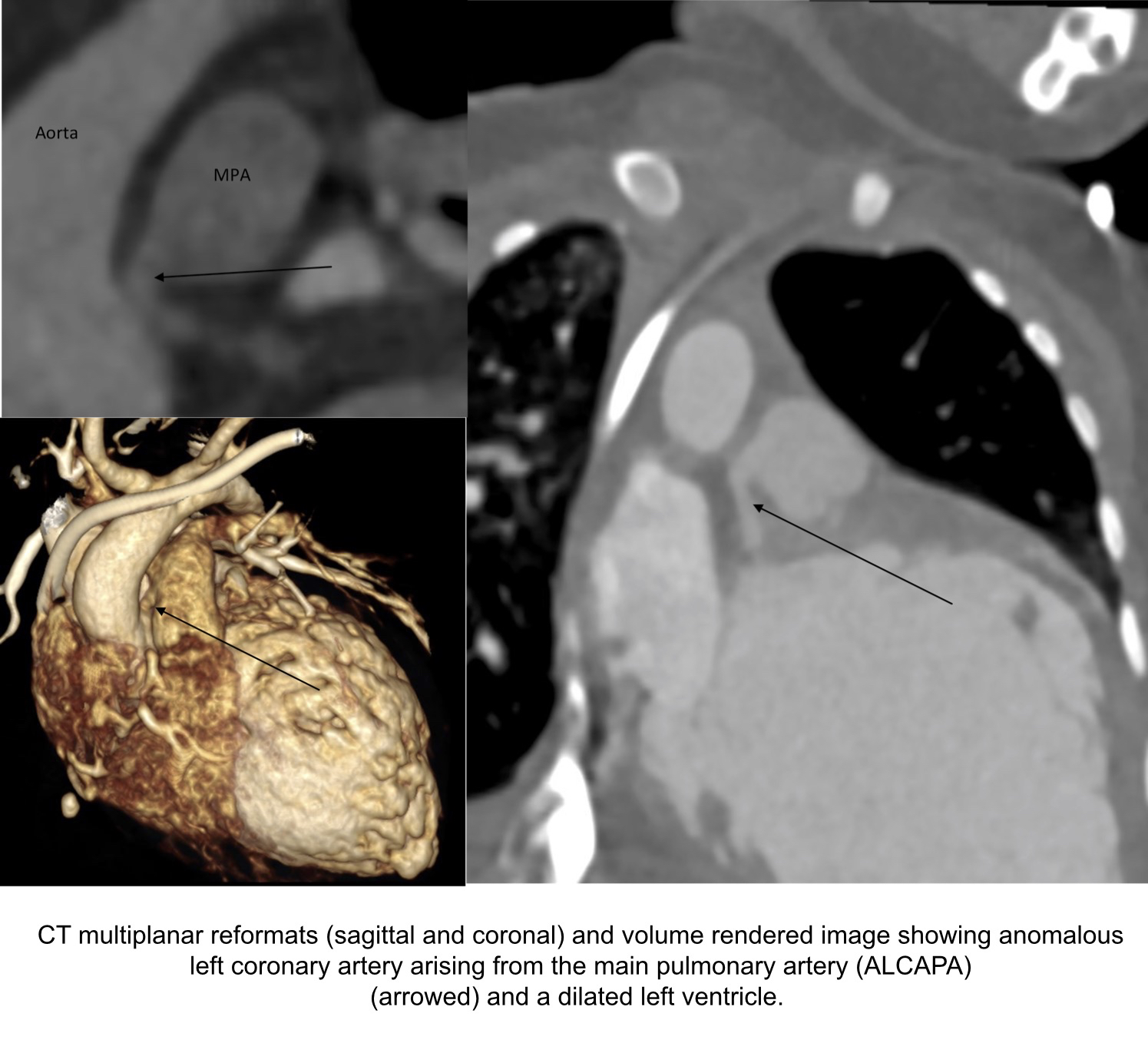
An 8-month old male born at term with known VACTERL association presented to his local hospital and a diagnosis of ischaemic cardiomyopathy and heart failure was made. Comorbidities included an imperforate anus, tracheoesophageal fistula, horseshoe kidney and nephrocalcinosis. The infant was transferred to the Freeman Hospital in Newcastle upon Tyne for further management of his severe cardiomyopathy of unknown etiology. The ECG appeared ischaemic. An echocardiogram revealed a dilated left ventricle with global left ventricular impairment and an ejection fraction of 27%. It was not possible to view the origin of the LAD at echocardiography. A CT coronary angiogram was performed which confirmed an anomalous left coronary artery arising from the pulmonary artery (ALCAPA). In utero, the pulmonary arterial and systemic arterial pressures are equal. Therefore, there is antegrade flow in both the normal RCA and the ALCAPA. After birth, the pulmonary arterial pressure and oxygen saturation drops, which results in the left ventricle being perfused by relatively desaturated blood under low pressure. Therefore, myocardial ischemia ensues [1]. The patient underwent cardiac surgery where the ALCAPA was re-implanted into the aorta. The patient was then transferred back to their base hospital for further management.
Questions
- The acronym VACTERL stands for vertebral defects, anorectal anomalies, cardiac defects, tracheoesophageal fistula, renal anomalies and limb anomalies. How many characteristic features need to be present to make the diagnosis?
- a)3
- b)4
- c)6
Answer – typically 3 features need to be present [2].
- What ECG findings are associated with ALCAPA?
- Widespread concave ST elevation
- LBBB and reduced voltage QRS complexes
- Abnormal Q waves in leads I, avL, V5, and V6, as well as by transient ST changes in these leads
Answer – The ECG findings associated with ALCAPA usually shows typical signs of an anterolateral myocardial infarction, manifested by abnormal Q waves in leads I, avL, V5, and V6, as well as by transient ST changes in these leads. 20-45% of patients do not show abnormal Q waves so the diagnosis should be strongly suspected if there is abnormal R wave progression in the chest leads [3].
References
[1] https://emedicine.medscape.com/article/893290-overview#a5
[2] https://ghr.nlm.nih.gov/condition/vacterl-association
[3] Electrocardiogram of anomalous left coronary artery from the pulmonary artery in infants. Hoffman JI, Paediatric Cardiology 2013 Mar;34(3):489-91


