An unusual cause of chest pain
Dylan Yong, Nadir Khan, Michelle Williams
Royal Infirmary of Edinburgh, University of Edinburgh
Case history
A 78-year-old female presented with chest pain of increasing frequency. She had undergone investigation of chest pain with invasive coronary angiography and balloon angioplasty to her left coronary artery 2 weeks prior.
Admission chest x-ray showed a right sided pleural effusion and an enlarged cardiac contour (Figure 1A). Her troponin and D-dimer were raised. Electrocardiogram (ECG) was unremarkable. She underwent a CT pulmonary angiogram (CTPA) which demonstrated a large pericardial effusion with maximum depth of 3.7cm (Figure 1B). Within this, there was an area of homogenous high attenuation in the epicardial space, following the course of right coronary artery. This was causing mass effect on the adjacent right atrium and ventricle. There was evidence of cardiac tamponade with straightening of the interventricular septum. Echocardiogram revealed a mass in the epicardial space suspicious for malignancy (Figure 1C).
A therapeutic pericardial drain was performed and haemoserous fluid obtained was sent for cytology. A total of 1.5 litres of fluid were drained from the right pleural space. Repeat CT post pericardial drainage demonstrated the mass more clearly (Figure 1D). Cytology from the pericardial effusion confirmed a diagnosis of primary cardiac diffuse large B cell lymphoma, stage IV. CT staging demonstrated no other sites of disease. Following discussion in a multi-disciplinary meeting, she received R-CHOP chemotherapy. She had an excellent response to the treatment, with a repeat 3-month interval CT scan demonstrating no measurable disease. (Figure 1E)
Discussion
Cardiac malignancy is rare, and primary cardiac lymphoma (PCL) accounts for only 1% of primary cardiac tumours.1 Amongst the small number of cases of PCL both B-cell and T-cell lymphomas have been reported.1 The majority of the PCL arise from the right side of the heart, particularly the right atrium.2 The reason for this distribution is unknown2. Cardiac involvement may also occur in up to 20% of patients who have diffuse nodal lymphoma.1 Lymphoma is an important differential diagnosis for cases when more than one cardiac chamber is involved.
Diagnosis of primary cardiac tumours is typically late and they are associated with a poor prognosis.2Symptoms are related to the site of involvement of the heart. Ikeda et al. reviewed the presentations of 40 patients with PCL and found that patients generally complain of non-specific symptoms such as dyspnoea and oedema, or present with arrhythmias and pericardial effusion.3
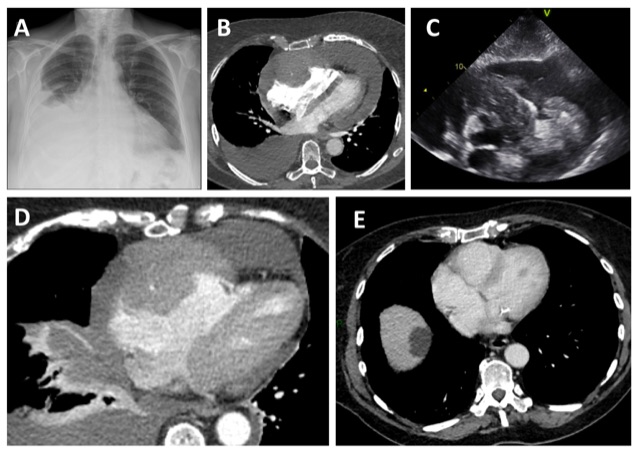
Figure Legend
Figure 1A. Chest X-ray with an enlarged cardiac contour and a right pleural effusion.
Figure 1B. CTPA showing a right pleural effusion and pericardial effusion. Homogenous material surrounding the right coronary artery causing mass effect on the right atrium and right ventricle.
Figure 1C. Transthoracic echocardiography showing a mass suspicious for malignancy in the epicardial space.
Figure 1D. CT of the chest after pericardial drainage showing the mass in the epicardial space.
Figure 1E. CT of the chest after treatment showing no evidence of residual disease.
Multiple-choice questions
1. What percentage of patients with diffuse nodal lymphoma have cardiac involvement?
- 5%
- 10%
- 20%
- 30%
- 40%
2. What is the name given to the appearance of a pericardial effusion on chest x-ray?
- Sillhouette sign
- Chang sign
- Water-bottle sign
- Double bubble sign
- Snowman sign
3. Which chemotherapy drug is correctly associated with the type of cardiovascular toxicity?
- Anthracycline – heart failure
- Cyclophosphamide – ischaemia
- Fluorouracil – hypertension
- Cisplastin – ischaemia, thromboembolism
- Vincristine – heart failure
Answers: 1/C, 2/C, 3/A
References
- Patel J, Melly L, Sheppard MN. Primar cardiac lymphoma: B- and T-cell cases at a specialist UK centre. Ann Oncol 2010; 21(5):1041-5
- Ceresoli GL, Ferreri AJ, Bucci E, Ripa C, Ponzoni M, Villa E. Primary cardiac lymphoma in immunocompetent patients: diagnostic and therapeutic management. Cancer 1997;80: 1497-1506.
- Ikeda H, Nakamura S, Nishimaki H, Masuda K, Takeo T, Kasai K, et al. Primary lymphoma of the heart: case report and literature review. Pathol Int 2004;54(3):187-95


