Multimodality imaging in a case of left atrial myxoma
Williams, MG1; Lewis, K2; MacIver, DH3; Sheffield, E4, Gosling, O3
- Department of Cardiology, Bristol Heart Institute, Bristol, UK
- Department of Radiology, Musgrove Park Hospital, Taunton, UK
- Department of Cardiology, Musgrove Park Hospital, Taunton, UK
- Department of Pathology, North Bristol NHS Trust, Bristol, UK
An asymptomatic 52-year-old gentleman was referred to our district general hospital for routine review due to a family history of aortopathy. He had no past medical history and was normotensive. An initial transthoracic echocardiogram (TTE) revealed normal left ventricular function and normal indexed aortic root dimensions.
He returned for a follow up scan 5 years later and he was found to have asymptomatic moderate LV systolic dysfunction on TTE. Cardiovascular magnetic resonance imaging (CMR) was arranged. This confirmed moderate left ventricular impairment (ejection fraction 43%), no regional wall motion abnormality, no late gadolinium enhancement, a bicuspid aortic valve and a mildly dilated aortic root (Figure 1A-B). There was no evidence of an intra or extra-cardiac mass. The patient was commenced on a beta-blocker and angiotensin receptor blocker.
Two years later (Figure 1C) a repeat TTE now demonstrated a large left atrial mass. He was admitted and a transoesophageal echocardiogram (Figure 1D) and a cardiac CT (Figure 1E-F) were performed which confirmed the presence of a 22 x 15 mm pedunculated left atrial mass attached to the interatrial septum. There was no evidence of metastases. The CT also confirmed normal coronary arteries. He was discussed with our local cardiothoracic centre and was transferred urgently for surgical resection (Figure 1G). He has made an excellent recovery and subsequent histological analysis confirmed this was a myxoma.
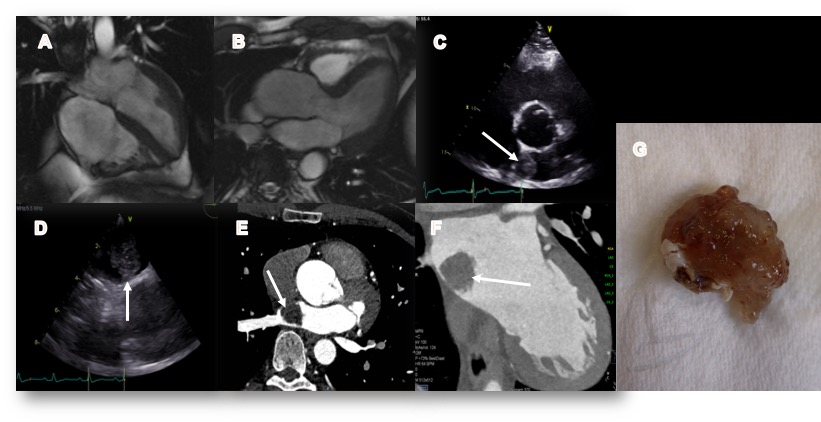
Figure 1: 4 (A) and 3 chamber (B) cardiac MRI images showing dilated aortic root and no evidence of atrial myxoma in 2015. C Subsequent transthoracic echocardiogram (2017) in the parasternal short axis showing echogenic lesion (white arrow) in the left atrium. D Transoesophageal echocardiogram (TOE) demonstrating the pedunculated lesion attached to the interatrial septum. Contrast-enhanced coronary CT angiogram showing the mass in the axial (E) and oblique (F) views. (G) Photograph of excised lesion prior to histological analysis
Multiple choice questions:
1. What is the median age of presentation of a myxoma?
A) 20-30 years
B) 30-40 years
C) 40-50 years
D) 50-60 years
E) 60-70 years
Answer C)
Cardiac myxomas are seen most frequently in adult females. At presentation, the median age is 49 years. However, cases have been reported in patients under 20 years and over 90 years of age1.
2. Which statement regarding myxoma is correct?
A) Myxoma is the most common type of tumour found in the heart.
B) Treatment is urgent due to high risk of fatal embolism and haemodynamic collapse
C) Local recurrence is common and affects >20% of cases
D) Roughly half of myxomas are solitary
E) The right atrium is the most common location
Answer B)
Metastatic tumours are 20-40 times more common than myxomas, which are the most common primary cardiac tumour2. Surgical excision should be considered in all patients as a matter of urgency. Death from embolic complications between diagnosis and treatment has been estimated at between 8-10%3. Local recurrence is rare affecting 3-4% of patients4. 90% of myxomas are solitary and the left atrium is the most common location representing 86% of myxomas1.
3. Which of the following statements regarding the appearance of a myxoma on CT is false?
A) They demonstrate high attenuation on non-contrast CT
B) 10% are calcified
C) Pedunculated appearance
D) Heterogeneous contrast enhancement
E) May be seen to prolapse through the mitral valve
Answer A)
Myxomas usually exhibit low attenuation on non-contrast CT. 10% may be calcified, more commonly when they are located in the right atrium. They are often pedunculated and attached to the interatrial septum via a stalk. They enhance heterogeneously due to the individual tumours’ chronicity and degree of necrosis and haemorrhage. Large tumours may prolapse through the mitral valve and can cause LV inflow obstruction2.
References:
1Mir IA et al. Atrial myxoma ‘a review’ International journal of community medicine and public health 2016 Jan; 3(1):23-29
2Kassop D et al. Cardiac Masses on Cardiac CT: A Review. Current Cardiovascular Imaging Reports. 2014;7(8):9281. doi:10.1007/s12410-014-9281-1.
3Dato GMA et al. Long term follow up of cardiac myxoma, (7-31years). Journal of Cardiovascular Surgery. 1993;34(2):114-43.
4Castells E et al. Cardiac myxoma: Surgical treatment, long term results and recurrence. J Cardiovasc Surg. 1993;34(1):49-53.
2Kassop D et al. Cardiac Masses on Cardiac CT: A Review. Current Cardiovascular Imaging Reports. 2014;7(8):9281. doi:10.1007/s12410-014-9281-1.
3Dato GMA et al. Long term follow up of cardiac myxoma, (7-31years). Journal of Cardiovascular Surgery. 1993;34(2):114-43.
4Castells E et al. Cardiac myxoma: Surgical treatment, long term results and recurrence. J Cardiovasc Surg. 1993;34(1):49-53.


