Authors: Dr Chrysovalantou Nikolaidou1, Dr Marian Lung2, Professor Stefan Neubauer1
-
Oxford Centre for Clinical Magnetic Resonance Research, University of Oxford, Oxford
-
Radcliffe Department of Medicine, John Radcliffe Hospital, Oxford
Case history
A 53-year-old woman, with no significant past medical history, was referred for cardiac MR Imaging (CMR) to further characterise a right atrial mass with imaging characteristics in keeping with cardiac myxoma on echocardiogram (Image 1), which was performed for worsening shortness of breath. Computed tomography revealed extensive lymphadenopathy and multiple lesions within the chest, abdomen, and subcutaneous soft tissue. The blood tests showed elevated white blood cell count with neutrophilia, iron deficiency anaemia, elevated platelet count, and significantly elevated CRP and D-dimers. The provisional diagnosis was cardiac myxoma in the context of possible Carney complex.
The CMR was performed on a 1.5T Magnetom Avanto (Siemens, Erlangen, Germany) scanner, using a dedicated protocol for cardiac masses, including cine imaging, tissue characterisation with T1- and T2-weighted imaging and parametric mapping, fat suppression, early and late gadolinium imaging, and rest perfusion imaging. CMR revealed a large, irregular-shaped mass (60 x 32 x 45 mm) attached to the lateral right atrial wall and adjacent to the basal-mid inferior and free right ventricular wall, and the right atrioventricular grove. The mass was protruding into and occupying most of the right atrial chamber. Due to the thin right ventricular and right atrial walls, it was difficult to clearly determine the extent of invasion of the mass into these walls. The signal characteristics of the mass were fairly homogeneous, with similar density to the myocardium on T1-weighted imaging and high signal on T2-weighted imaging (Image 2). There was minimal contrast uptake on first-pass perfusion imaging, with minimal heterogeneous enhancement on late gadolinium imaging (Image 3). There was also a second, slightly irregular mass (32 x 25 mm), with similar imaging characteristics, adjacent to the outside of the lateral left atrial wall and left atrioventricular groove.
Overall, the findings were in keeping with a malignant tumour, which, in combination with the widespread disease identified on computed tomography, were most likely to reflect metastatic cardiac involvement from sarcoma or melanoma. The histopathological and molecular investigations on the biopsy samples taken from lymph nodes from the neck and from axilla tissue showed evidence of metastatic melanoma, with little chances of response to systemic treatment. It was clear that the tumour was inoperable, and that the best management was palliative care. The patient died three weeks after the CMR scan.
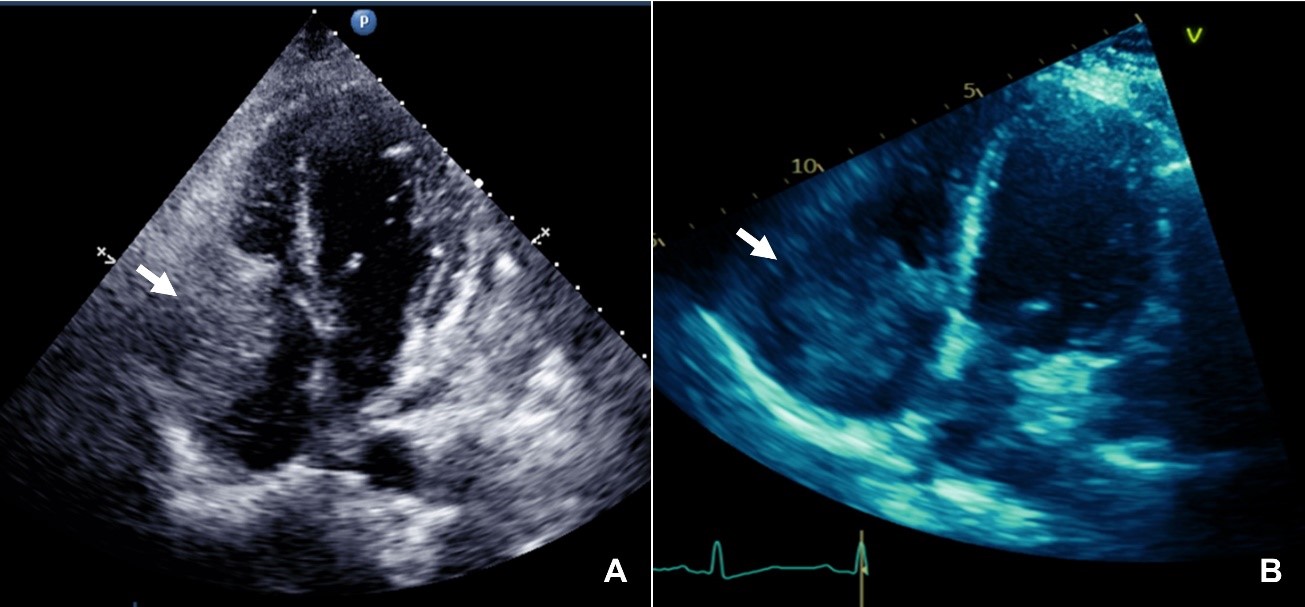
Image 1. Apical four-chamber view (A) and right-ventricular focused view (B), showing a right atrial mass attached to the lateral right atrial wall and protruding into the right ventricle through the tricuspid valve.
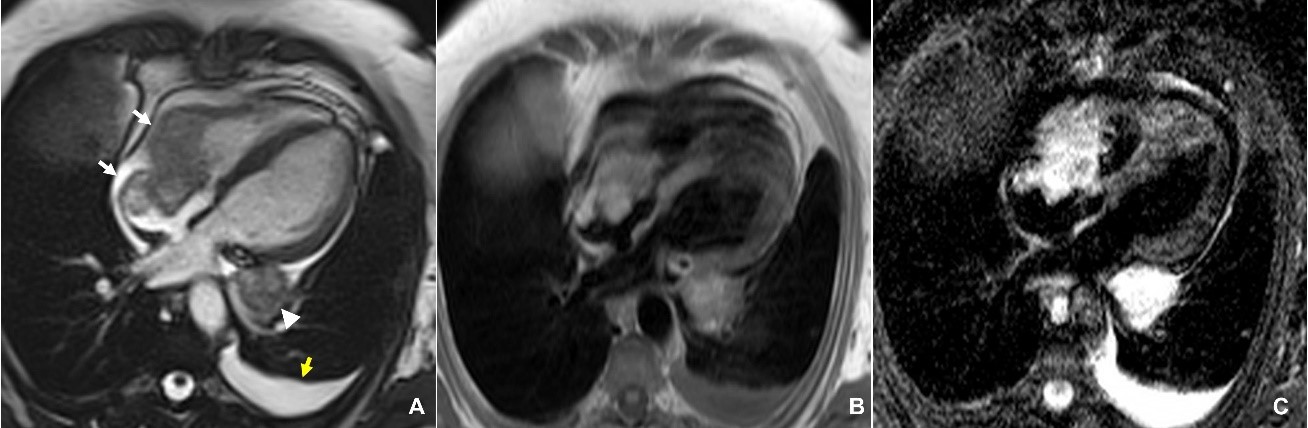
Image 2. Horizontal long-axis view of the heart on a still frame from cine steady-state free precession (SSFP) imaging, showing the large irregular right atrial and right ventricular mass (white arrows), a second mass in the basal lateral left ventricular wall (arrowhead), and a small left pleural effusion (yellow arrow) (A). The masses have fairly homogeneous signal, similar to the myocardium on T1-weighted imaging (B), and high signal on T2-weighted imaging. The pleural effusion also appears bright on T2-weighted imaging.
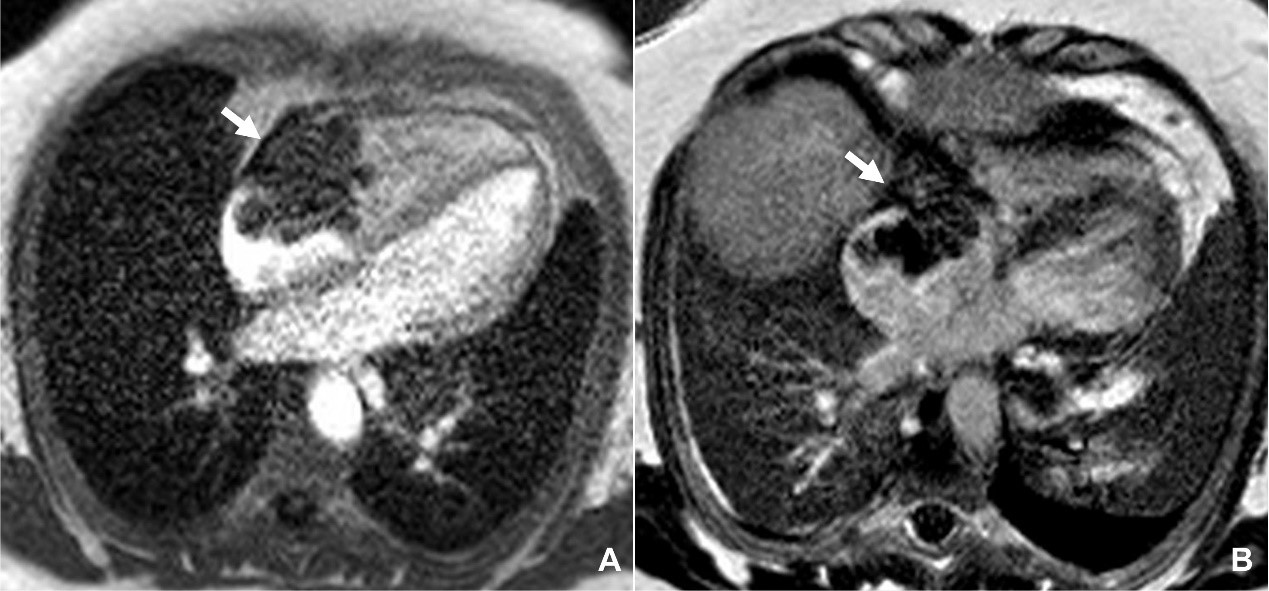
Image 3. Horizontal long-axis view of the heart showing minimal contrast uptake of the mass (white arrow) on first-pass perfusion imaging (A), and minimal heterogeneous enhancement on late gadolinium imaging (B).
Questions
- Which of the following statements is true?
- The majority of primary cardiac tumours are benign
- Primary cardiac tumours are more common than cardiac metastases
- The most common benign cardiac tumours are haemangiomas and teratomas
- The most common malignant cardiac tumours are sarcomas and lymphomas
Answers: A, D
2. The clinical manifestation of cardiac tumours can include:
- Obstruction
- Pericardial effusion
- Embolic events
- All of the above
Answer: D
- Which features on CMR imaging are suspicious for a malignant mass?
- Large size
- Left-sided cardiac location
- Tissue inhomogeneity
- Low signal on first-pass perfusion imaging
Answers: A, C
Discussion
Cardiac tumours represent a rare pathology, with an estimated prevalence of only 0.002%–0.3% at autopsy. Approximately 75% of primary cardiac tumours are benign, with more than half of these being myxomas. The majority of the malignant primary cardiac tumours are sarcomas and lymphomas. However, metastatic involvement of the heart is more common than primary cardiac tumours, with melanoma, lymphoma, and carcinoma of the lung, breast, and oesophagus being the most frequent initial source. Cardiac tumours can potentially involve any of the cardiac structures and have a diverse clinical presentation, which includes systemic manifestations, symptoms due to mass effect, or embolic events.
While echocardiography remains the first line diagnostic imaging test, CMR has emerged as a powerful diagnostic tool in the diagnosis of many cardiac pathologies, including cardiac masses. CMR can differentiate normal structures (‘pseudotumours’) or cardiac thrombi from abnormal lesions, benign from malignant masses, and provide non-invasive tissue characterisation with the late gadolinium enhancement (LGE) technique, but also with the new T1 and T2-mapping sequences. Imaging features suggestive of a malignant cardiac mass include large size, infiltration of adjacent structures, inhomogeneity on tissue characterisation, right-sided cardiac location, significant contrast uptake on first-pass perfusion imaging, and concomitant pericardial or pleural effusion. However, precise histological assessment is not possible, and pathology remains the gold standard for the accurate diagnosis of the type of a mass, especially in the case of malignant masses. Another advantage of CMR is the ability to assess the vascularity of a mass, its extension, and the relationship to nearby structures, thus helping to guide treatment and assess feasibility of surgical resection.
In conclusion, CMR can reliably evaluate the location, size, and extent of cardiac masses, as well as their invasion across tissue planes. With its unique capability of non-invasive tissue characterisation, CMR can help differentiate between primary and secondary tumours, and provide important clues as to the differential diagnosis.
References
- Burazor I, Aviel-Ronen S, Imazio M, et al.Metastatic cardiac tumors: from clinical presentation through diagnosis to treatment. BMC Cancer 2018; 18: https://doi.org/10.1186/s12885-018-4070-x.
- Cardiac tumors. EACVI 3D Echocardiography Box. https://www.escardio.org/Education/Practice-Tools/EACVI-toolboxes/3D-Echo/cardiac-tumors.
- Hoffmann U, Globits S, Schima W, et al. Usefulness of magnetic resonance imaging of cardiac and paracardiac masses. Am J Cardiol 2003; 92(7): 890–895.
- Motwani M, Kidambi A, Herzog BA, Uddin A, Greenwood JP, Plein S. MR imaging of cardiac tumors and masses: a review of methods and clinical applications. Radiology 2013; 268(1): 26-43. doi: 10.1148/radiol.13121239. PMID: 23793590.
- Mousavi N, Cheezum MK, Aghayev A, et al. Assessment of Cardiac Masses by Cardiac Magnetic Resonance Imaging: Histological Correlation and Clinical Outcomes. Journal of the American Heart Association 2019; 8(1): e007829.


