An unusual cause of extensive bilateral lower limb oedema
Rachael Forsythe and Orwa Falah, Edinburgh
An 84 year old male presented with sudden onset massive bilateral lower limb swelling and a 4 day history of vague abdominal pain and swelling. He had no previous similar episodes; otherwise fit and well. Still working as a farmer. Treated for hypertension (bisoprolol), atrial fibrillation (recently commenced on apixaban) but no other relevant past medical history. No personal or family history of thrombophilia. He was haemodynamically stable on admission. Relevant bloods: Hb 118, platelets 160, creatinine 169, urea 16.6, eGFR 33.
Urgent CTA was performed (images 1-3).
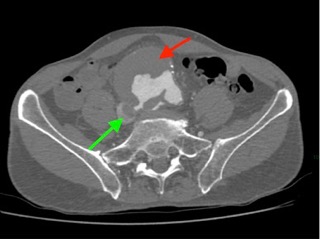
Image 1: Large AAA (red arrow) rupturing into IVC (green arrow) via aorto-caval fistula.
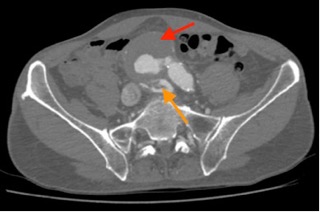
Image 2: Contrast from the AAA (red arrow) is seen within the inferior vena cava and iliac veins (orange arrow)

Image 3: Contrast from the AAA (red arrow) is seen within the inferior vena cava (green arrow), which also contains thrombus (blue arrows)
Question 1:
What are the diagnoses?
Question 2:
What effect does acute renal failure have on apixaban clearance?
- a.no effect – apixaban does not undergo renal excretion and would therefore be cleared within 48 hours
- b.increases the clearance time; dose should be reduced if serum creatinine >133micromol/litre or age >80 or weight <61kg
- c.increases the clearance time by an extra 72 hours but only when the eGFR is below 30
Question 3:
Why might a patient with aorto-caval fistula present with breathlessness and syncope?
- a)aorto-caval fistula can cause a left-to-right shunt resulting in high output congestive cardiac failure
- b)breathlessness and syncope is a manifestation of haemorrhagic shock
- c)they may develop acute aortic stenosis due to elevated right ventricular systolic pressure
The optimal approach to this would be urgent open repair, however in the context of acute renal failure, apixaban assay confirmed that clearance was markedly reduced. It was therefore not felt safe to proceed with open repair in the acute period due to the risk of being unable to achieve haemostasis. The patient therefore had a trans-jugular inferior vena caval filter inserted followed by standard EVAR the following day (image 4).

Image 4: 3D reconstruction following EVAR (thick green arrow), with IVC filter visible (thin green arrow)
Despite successful EVAR deployment, the fistula remained patent with a type 2 endoleak due to patent lumbar arteries. However, renal function rapidly returned to normal and the patient experienced rapid symptomatic relief. He was discharged home on warfarin with plans for early follow up imaging.
Answers:
- Ruptured abdominal aortic aneurysm with large aorto-caval fistula and concurrent bilateral ilio-femoral DVTs extending into the IVC
- B
- A


