Single Coronary Artery System or a Very Hyperdominant Left Circumflex?
Authors and affiliations:
1. Uzma Gul
Cardiology Registrar , Russells Hall hospital
2. Robert Hugget
Consultant Cardiologist, Russells Hall hospital
3. Min Yen Wong
Consultant Radiologist, Russells Hall hospital
4. Nazia Kaushal
Consultant Radiologist, Russells Hall hospital
Case Report
A 63 year old female presented with atypical angina. Physical examination was unremarkable.
Electrocardiogram was normal and the echocardiogram revealed a structurally normal heart.
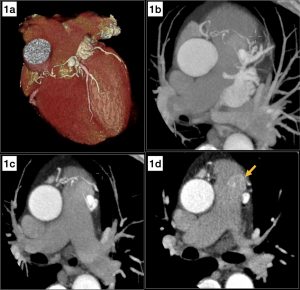
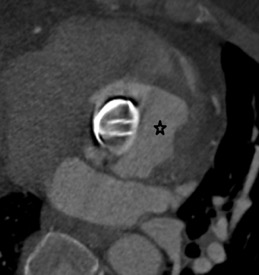
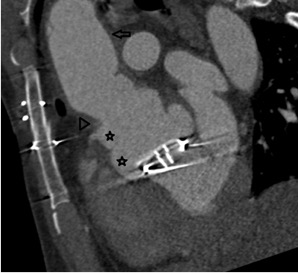
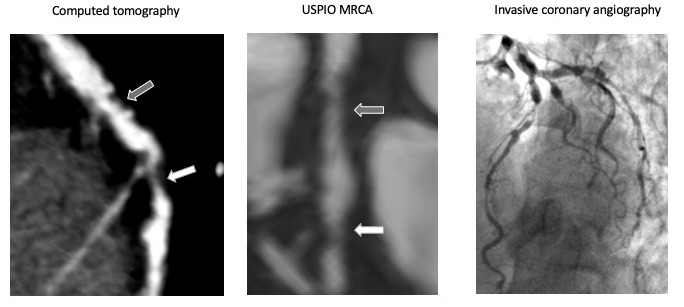
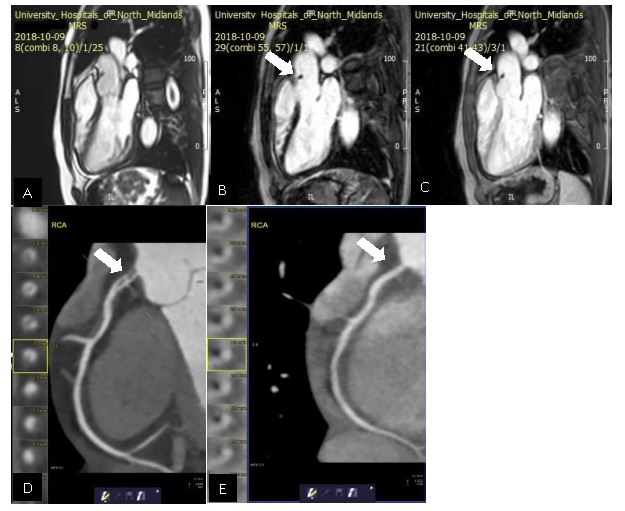
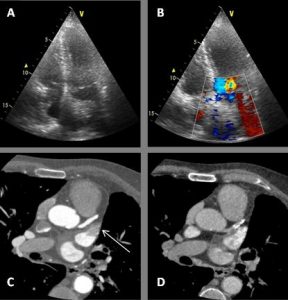
CT coronary angiography was performed and is presented below.
Images
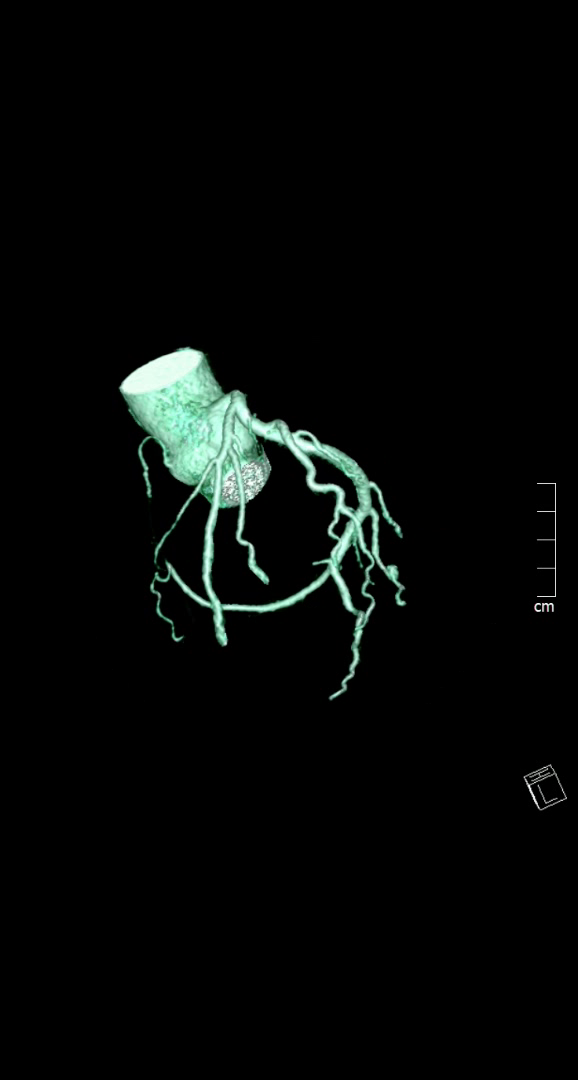
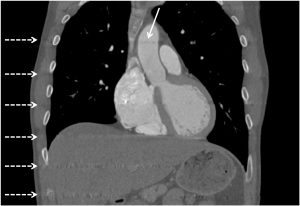
Image 1- 3D coronary tree reconstruction frontal view
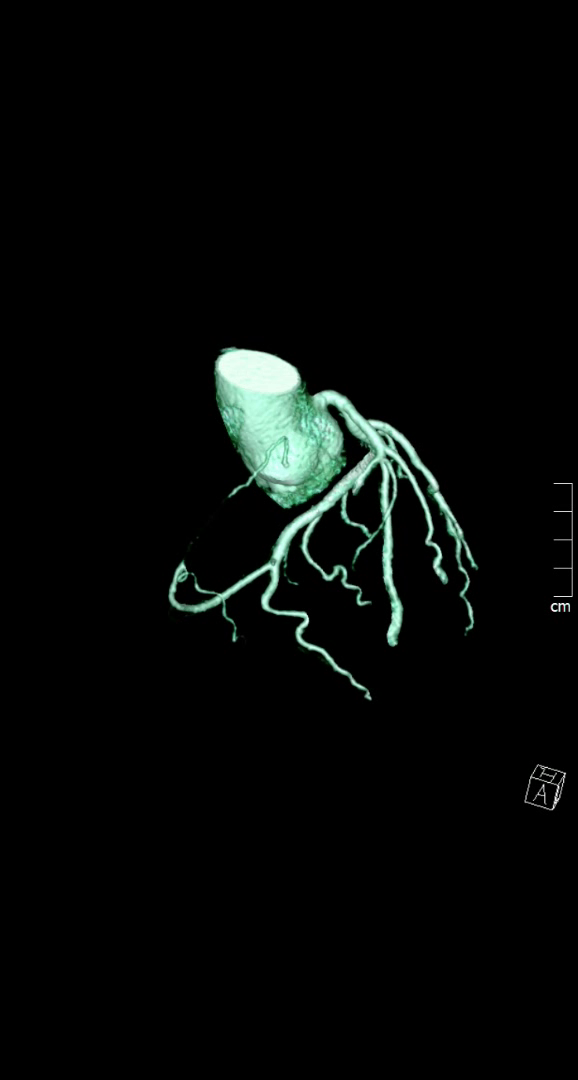
Image 2-3D coronary tree reconstruction lateral view
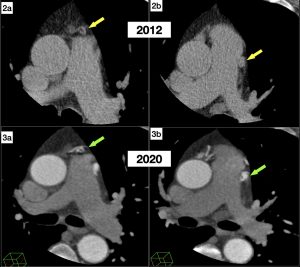
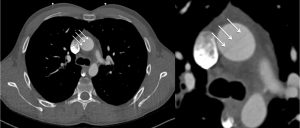
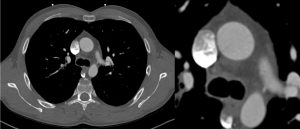
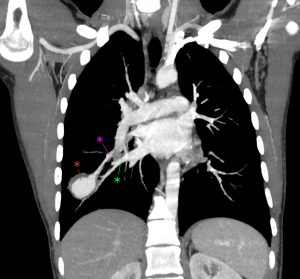
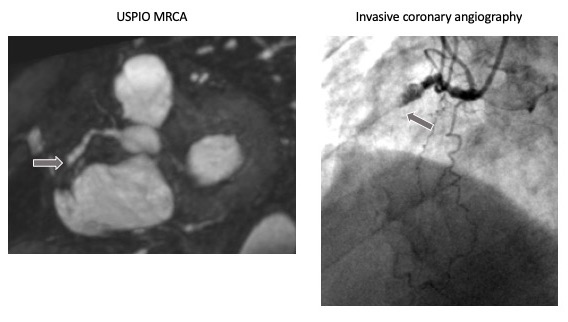
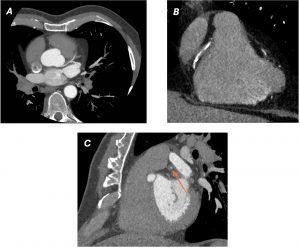
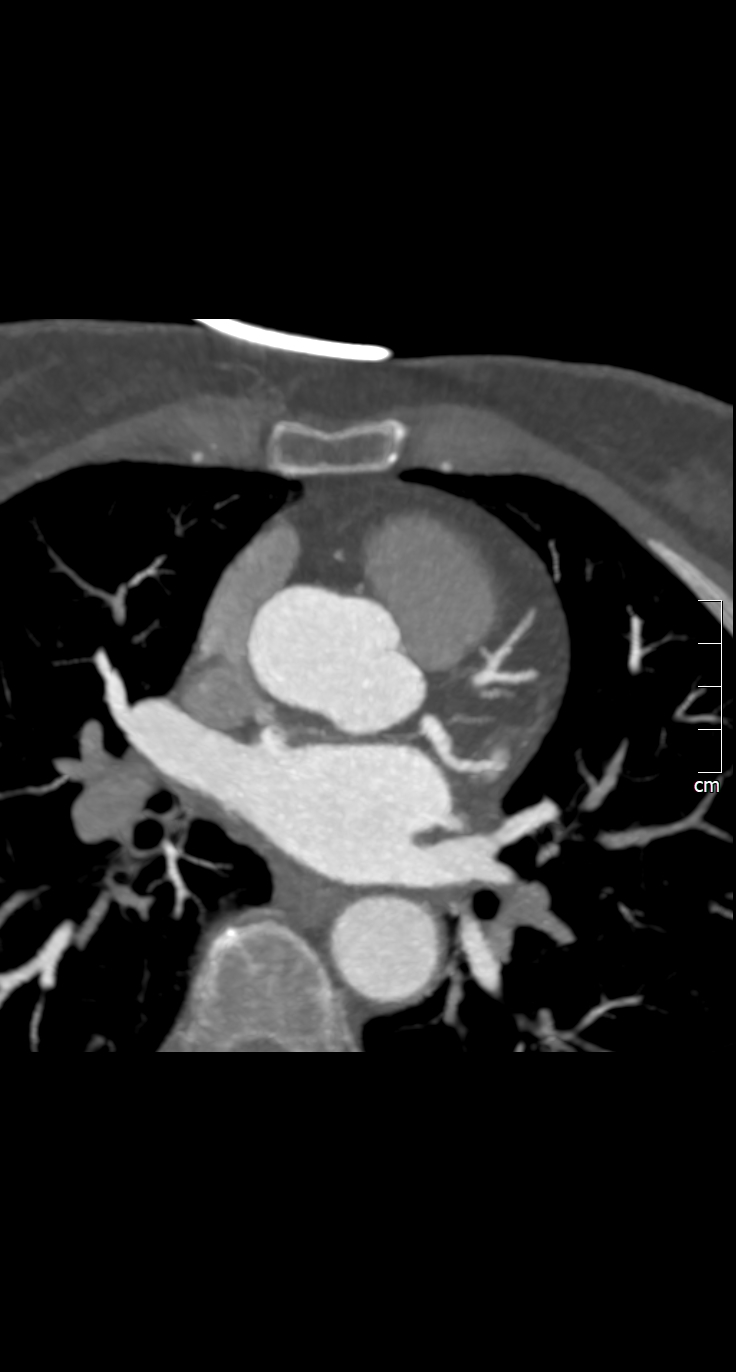 Image 3- Nodal artery arising from LCX
Image 3- Nodal artery arising from LCX
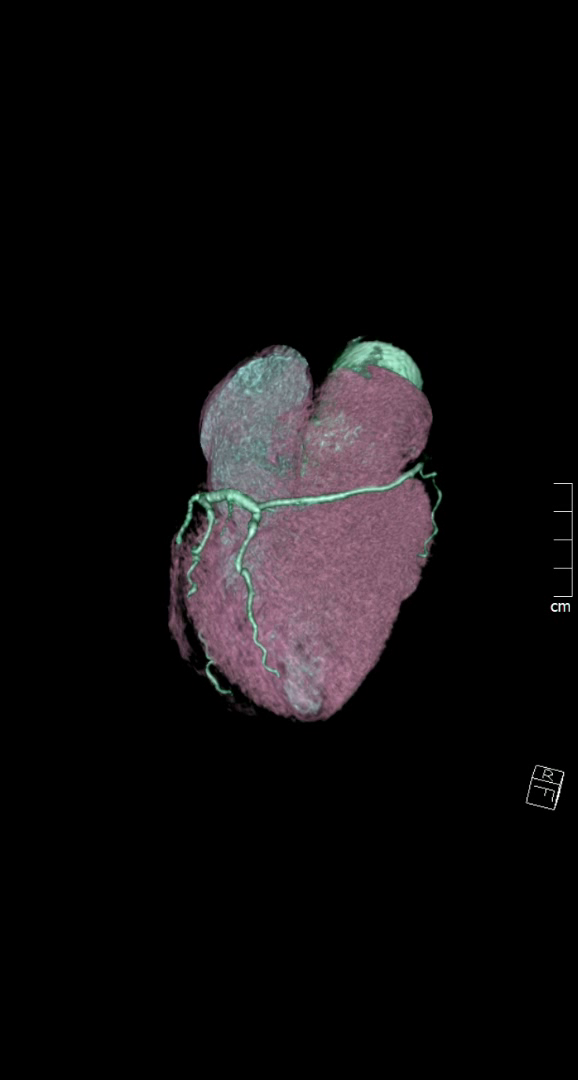
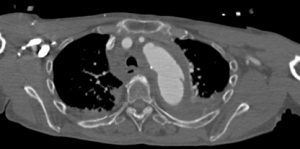
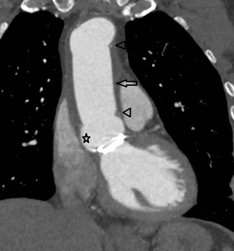
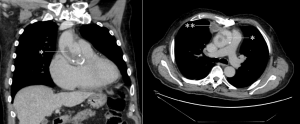
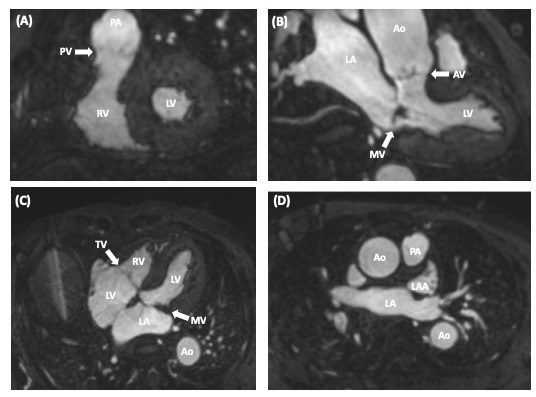
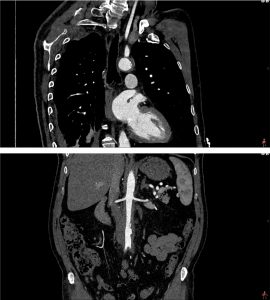
Image 4- 3D whole heart reconstruction
Questions & Best answers
I) What is the mechanism of ischemia in SCA?
1. Slit-like ostium & ostial ridge/ acute-angle takeoff
2. coronary spasm/ hypoplasia/ tortuous anatomy
3. Interarterial course with exercise-related narrowing
4. Intramural course with lateral compression
5. All of above
II) In Lipton classification
1. First alphabet represents the sinus of origin
2. Roman numerals represents anatomical distribution
3. Letters A,B,P,S, C represent course with reference to great vessels
4. All of above
III) Which of following congenital heart conditions are associated with single coronary artery?
1. Bicuspid aortic valve
2. Hypertrophic cardiomyopathy
3. Atrial septal defect
4. Tetrology of fallot
5. Ebstein anomaly
Answers
I) 5
II) 4
III) 1, 2 &4
Discussion
Single coronary artery (SCA) is described as an anomaly where one coronary artery originates
from a single coronary ostium from aorta and supplies the whole heart. 1 SCA is a rare anomaly
with prevalence of 0.024–0.066% in structurally normal hearts. 2 Using the Lipton classification
of SCA, our case would be best described as a type L-I SCA. 3 Type L-I is usually believed to be
benign type SCA, some malignant types are associated with sudden cardiac death. 3
However by convention, our case may also be argued as not being a single coronary artery,
since RCA had a separate ostium from aorta. Although, it did not give any of its usual branches
and ended shortly after its origin, acting as hypoplastic or atretic. Hypoplastic coronary
however, by definition, is a congenitally underdeveloped coronary with absence of
compensatory collateral vessels. 4 By contrast, in our case RCA territory was supplied by LCx
continuation into the right AV groove.
Alternatively, one may argue it as a hyper-dominant LCx with a vestigial RCA. 5 The
Hyperdominant LCx has been described in literature as supplying the apex in addition to RCA
territory. 5 None of the LAD territory was supplied by LCx in our case however.
The coronaries were free of any plaque or stenosis in our case. The patient was managed
conservatively and had an uneventful course over nine months follow-up. There are case
reports of patients presenting with angina and found to have single coronary system but no
significant atherosclerotic stenosis. 2,6 On the other hand, most case reports with
hyperdominant coronary did have an atherosclerotic stenosis explaining presentation with
angina. 5
Learning points/take home messages
1. Both single coronary artery and hyperdominant coronary are rare but can have
important implications in planning treatment.
2. SCA can present with angina or sudden death without coronary stenosis.
3. CTCA giving three dimensional anatomical data and details beyond luminography is
especially useful.
Keywords: Absent right coronary artery, Hyperdominant left coronary, Single coronary artery
anomaly.
References
1. Ayman Elbadawi, BasaratBaig, Islam Y. Elgendy. Single Coronary Artery Anomaly: A Case
Report and Review of Literature. CardiolTher. 2018 Jun; 7(1): 119–123.
2. Prashanth Panduranga, abdulla AmourRiyamia. Single coronary artery from right aortic
sinus in a very elderly patient. Journal of the Saudi Heart Association. 2016; 28(4):257-
260
3. Sinha SK, Aggarwal P, Mishra V, et al. Unusual trifurcation of a single left coronary
artery. Case Reports 2018;2018:bcr-2017-222213.
4. Selma Kenar Tiryakioglu, Hakan Ozkan, Hakan Bahadir, et al. Left Main Coronary Artery
Hypoplasia in Elderly. Case Reports in Cardiology 2016; 2016: Article ID 4156581.
http://dx.doi.org/10.1155/2016/4156581
5. Agrawal N. Superdominant left-circumflex artery supplying significant proportion of RCA
and LAD territory. Case Reports 2015;2015:bcr2015210365.
6. Gitsios Gitsioudis,Evangelos Giannitsis, Waldemar Hosch, et al. Single coronary artery
with anomalous rising of the right coronary artery: a rare coronary anomaly diagnosed
by 256-multidetector computed tomography. Case reports in medicine. 2011; 2011:
108709. PMC3205733. doi:10.1155/2011/108709.