When a curry gives you more than heartburn: A rare cause of myocardial infarction.
Dr. S. Ahmed, Dr. A. Appaji, Dr. A. Large, Dr. S. Duckett Department of Cardiology, Royal Stoke University Hospital, Stoke-on-Trent.
A fifty-six year old female was admitted to accident and emergency (A&E) with a witnessed collapse at home. She had a background history of recurrent urinary tract infections and an eleven pack year history of smoking. She had diarrhoea and vomiting for two days prior to admission after having a home-cooked curry and recalled feeling dizzy and nauseous with chest discomfort before passing out.
On arrival to A&E, her blood pressure was 88/62 mmHg with symptoms of feeling light-headed and clammy. On examination her jugular venous pressure was elevated, normal heart sounds and bibasal crepitations on chest auscultation. Electrocardiogram (ECG) showed normal sinus rhythm with ST segment depression in leads III, aVF and V4 to V6 with a subsequent troponin rise of > 50000. CXR showed evidence of pulmonary oedema.
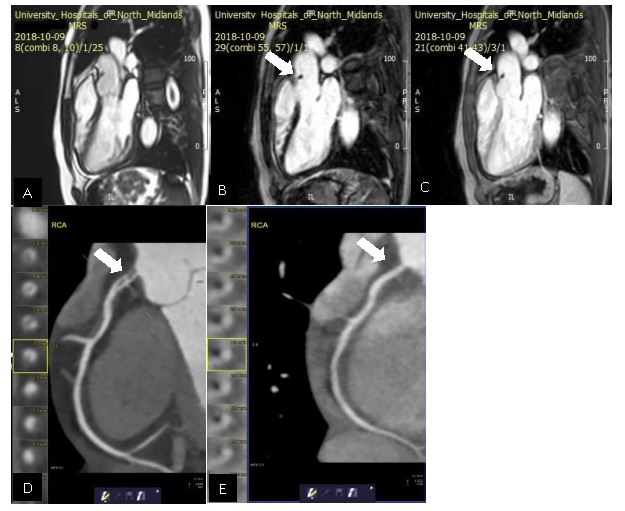
A cardiac MRI was performed which showed mild impairment of left ventricular function, a limited basal infero-septal myocardial infarction. An incidental finding of a small (5X8mm) mobile mass was seen in the proximal ascending aorta, fixed to the aortic wall superior to the ST junction and above the RCA origin which was felt to be thrombus. It was dark on the early gadolinium image (image C) and non-enhancing on the late gadolinium (image B).
CT coronary angiography was performed to further assess the coronary arteries which revealed a dissection flap (image D see arrow) causing moderate stenosis at the right coronary artery (RCA) ostium with further mild stenosis caused by a long soft tissue plaque in the proximal vessel. The images and cases were discussed with the interventional cardiology team and conservative management was felt to be the best option.
The patient was discharged with dual antiplatelet therapy for 12 months and an ACE inhibitor, statin and beta blocker. A follow up CT imaging revealed resolution of the RCA ostial dissection flap with no significant stenosis. (image E see arrow)
Discussion:
Spontaneous coronary artery dissection is a rare cause of non-atherosclerotic myocardial infarction with an incidence of 0.1% to 0.4% of all acute coronary syndromes.1 It is more commonly described in young females and known to be associated with fibromuscular dysplasia, connective tissue disease and peri-partum status. Frequently identified triggers include catecholamine release mediated by physical exertion, intense emotional stress and increased abdominal pressures induced by coughing, retching or vomiting.2 Both these mechanisms increase the shearing stress on the coronary artery wall. A conservative approach towards management with standard medical therapy is usually preferred compared to invasive angiography as most cases resolve spontaneously.
References:
1. Mortensen KH, Thuesen L, Kristensen IB, Christiansen EH. Spontaneous coronary artery dis- section: a Western Denmark Heart Registry study. Catheter Cardiovasc Interv. 2009 Nov 1;74(5):710-7.
2. Saw J, Aymong E, Sedlak T, Buller CE, Starovoytov A, Ricci D, Robinson S, Vuurmans T, Gao M, Humphries K, Mancini GB. Spontaneous coronary artery dissection: association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ Cardiovasc Interv. 2014 Oct;7(5):645-55.


