Authors:
Shubham Garg1, Ruhani Bali1, Akash Batta1, Bishav Mohan1, Shitij Chaudhary1
Affiliation:
Department of Cardiology, Dayanand Medical College and Hospital, Ludhiana, India
Case Summary:
A 49-year-old male with no prior comorbidities presented to the emergency room (ER) with a 7-day history of fever, cough and shortness of breath. On admission, the patient had a blood pressure of 80/56 mmHg, a heart rate of 120 bpm, a respiratory rate of 36/minute, elevated jugular venous pressure, clear lung fields and muffled heart sounds on auscultation. An electrocardiogram was done, which showed sinus tachycardia with low-voltage QRS complexes. A screening bedside echocardiogram showed a large pericardial effusion (maximum thickness of 28 mm) with right ventricular diastolic collapse, suggestive of tamponade physiology. A bedside echocardiography-guided pericardiocentesis was attempted in the ER. Initially, 15 ml of haemorrhagic fluid was drained, after which no further fluid was drained. Cardiology consultation was obtained, and the patient was transferred to the cardiac catheterization laboratory.
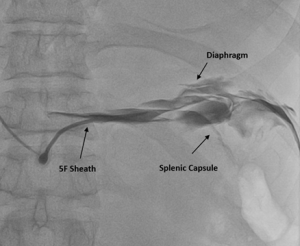
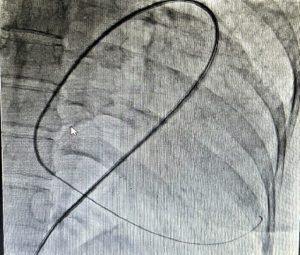
Fluoroscopy was done, and the sheath was found to be in the splenic capsule (Figure 1). Under fluoroscopic guidance, a pigtail was inserted over a 0.035” J-tipped Terumo wire, after confirming the position of the wire in the pericardial space (Figure 2), and 250 ml of pericardial fluid was drained. Post-pericardiocentesis, the patient was vitally stable.
Learning Points:
- Pericardiocentesis must always be done under fluoroscopic or expert echocardiographic guidance; blind procedures must be avoided.
- The position of the needle must always be confirmed once it enters the pericardial space.
Multiple Choice Questions:
- Which of the following clinical signs is not characteristic of cardiac tamponade?
- Jugular venous distension
- Muffled heart sounds
- Clear lung fields
- Bradycardia
- Pulsus paradoxus
- Which of the following signs on echocardiography does not support the diagnosis of cardiac tamponade?
- RV diastolic collapse
- RA systolic collapse
- Dilated IVC
- Swinging heart
- Decreased respiratory flow variation across the tricuspid valve
- Which of the following is the most appropriate management for a patient presenting with cardiac tamponade?
- Blind bedside pericardiocentesis
- Fluoroscopy-guided pericardiocentesis
- Intravenous fluids
- Clinical monitoring
- Intravenous diuretics
Answers: d, e, b


