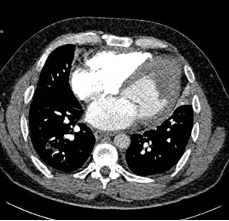

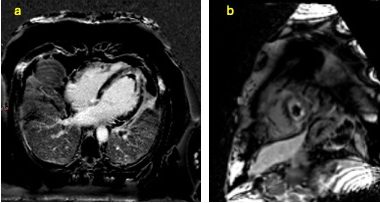
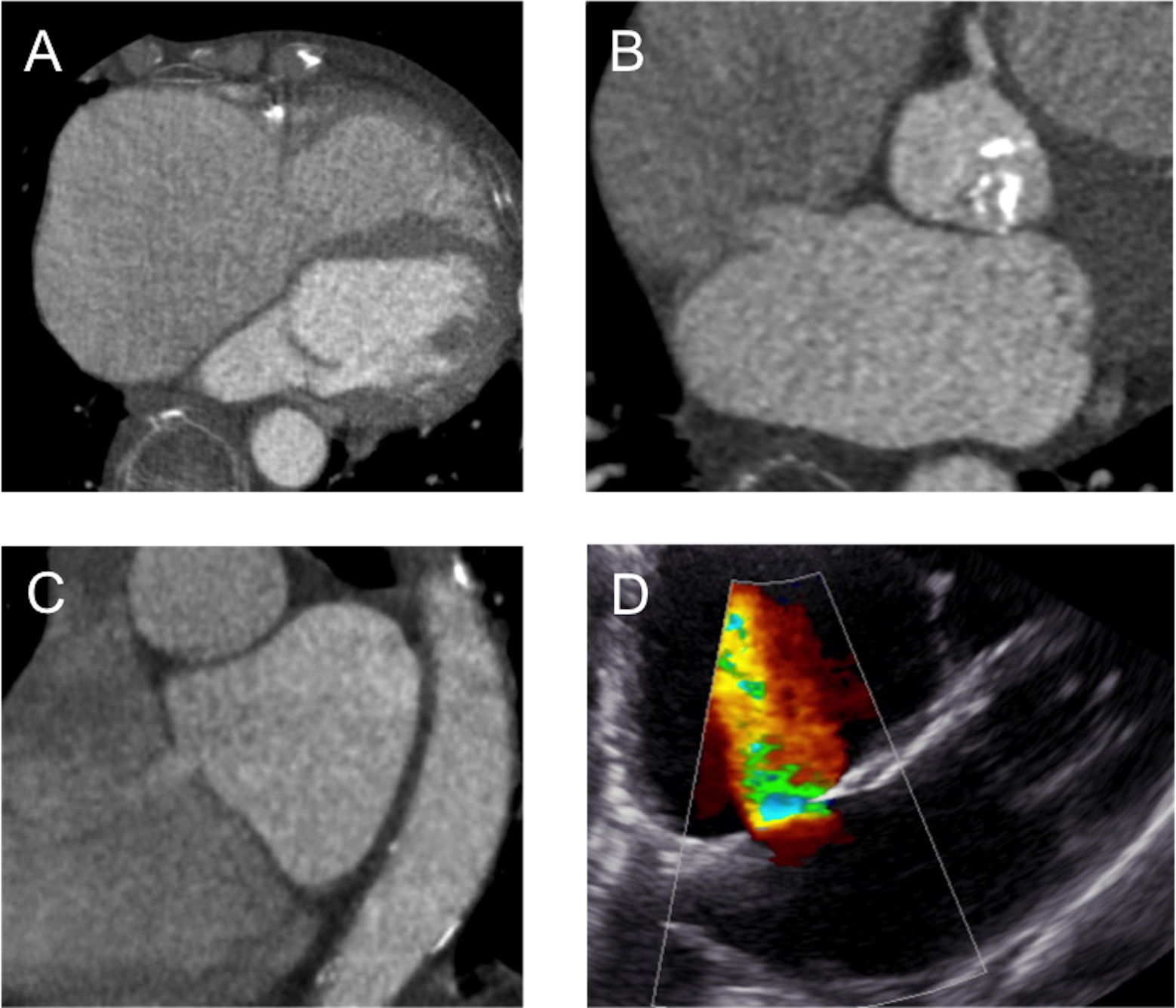
An 86 year-old male presented with progressive shortness of breath on exertion on a background of severe aortic stenosis. Cardiac computed tomgraphy demonstrated a hypertrophied left ventricle with a severely dilated right atrium (Figure A). Axial and sagittal multi-planar reconstructions revealed an ostium secundum atrial septal defect (ASD) with transit of contrast from the left to right atrium (Figure B and C). Transthoracic echocardiography confirmed a left-right shunt through the ostium secundum ASD (Figure D).
Ostium secundum ASDs are the most common type of ASD accounting for 80-90% of defects in the interatrial septum [1]. Shunt flow occurs predominantly during ventricular diastole with the direction of flow determined by difference in the compliance and capacity between the left and right ventricles [2]. Cardiac computed tomography acquisitions during late-diastole with opacification of the left heart can visualise ASDs without the requirement for the Valsalva manoeuvre.
In elderly patients with ostium secundum ASDs, larger left-right shunts may occur following changes in left ventricular compliance. In this case, the shunt acts as a ‘release valve’ for the left atrium to maintain lower pulmonary venous pressures. Closure of the defect may lead to an acute rise in left atrial pressure and precipitate pulmonary oedema.
References
[1] Johri AM, Rojas CA, El-Sherief A, et al. Imaging of the atrial septal defects: echocardiography and CT correlation. Heart. 2011;97:1441-1453.
[2] Sommer RJ, Hijazi ZM, Rhodes Jr. JF. Pathophysiology of Congenital Heart Disease in Adults. Part I: Shunt Lesions. Circulation. 2008;117:1090-1099.