Authors:
Dr Elizabeth Anderson, Dr Douglas Turner
Affiliations: Sheffield Teaching Hospitals NHS Foundation Trust
Case Summary
An adult male with extensive ischaemic heart disease underwent cardiac CT as part of pre-procedural planning for ventricular tachycardia (VT) ablation. His medical history included prior myocardial infarction treated with percutaneous coronary intervention and multiple coronary stents. He also had multiple cardiovascular co-morbidities including hypertension, hypercholesterolaemia and peripheral vascular disease. Despite guideline-directed heart failure therapy, his left ventricular ejection fraction remained reduced at approximately 35%, and he had previously received a dual-chamber implantable cardioverter-defibrillator (ICD) for primary prevention.
The patient had recently experienced ventricular fibrillation with appropriate ICD shocks and was therefore referred for consideration of VT ablation and underwent a planning cardiac CT to evaluate coronary anatomy, cardiac morphology and relevant structures, and substrate mapping prior to the anticipated electrophysiological procedure.
Imaging Findings
VT ablation planning CT protocol was used which included gated non-contrast, arterial phase and venous phase CT with split bolus contrast.
CT coronary angiography demonstrated previously placed coronary stents within the major epicardial vessels. There was no significant in-stent stenosis or obstructive disease identified within the coronary vessels.
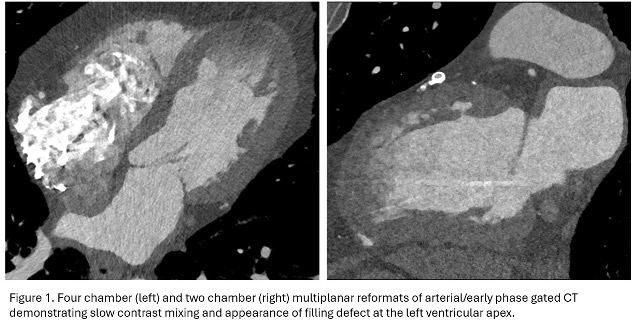
During arterial phase imaging, an apparent regional apical chamber filling defect was noted within the left ventricular apex, raising suspicion for possible left ventricular thrombus (Figure 1). Given the patient’s history of prior myocardial infarction and reduced left ventricular systolic function, this represented a clinically relevant consideration.
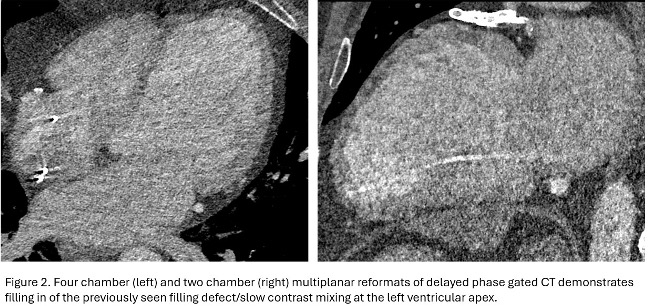
On the delayed acquisition however, the previously observed apical filling defect demonstrated opacification with contrast, with complete filling of the region (Figure 2). No persistent low attenuation intracavitary mass was identified. These appearances were therefore consistent with delayed contrast mixing within the apical cavity, owing to altered flow dynamics, rather than intra-cavitary thrombus. The slow contrast medium admixing was considered likely related to regional wall motion abnormality in the context of prior ischaemic injury.
Discussion
Left ventricular thrombus is a recognised complication in patients with prior myocardial infarction and impaired left ventricular systolic function, particularly in the presence of apical akinesis or dyskinesis (1). Accurate identification is important given the associated risk of systemic embolisation and the potential need for anticoagulation.
However, poor ventricular function with abnormal intracavitary blood flow can produce apparent filling defects on arterial phase CT imaging, particularly in regions with abnormal contractility. In such cases, incomplete contrast mixing may mimic thrombus and lead to diagnostic uncertainty, a phenomenon also well described in the left atrial appendage.
Delayed phase imaging provides a useful technique for differentiating true thrombus from pseudo-defects caused by slow/abnormal flow (2). True thrombus typically remains as a persistent low-attenuation mass that does not enhance on delayed images, whereas filling defects secondary to slow contrast medium admixing demonstrate progressive contrast equilibration, with resolution of the apparent filling defect. Cardiac MRI is a highly sensitive alternative imaging modality, with thrombus appearing as a non-enhancing mass on late gadolinium imaging.
This case highlights the importance of delayed phase imaging when an apparent left ventricular filling defect is identified on CT coronary angiography, improving diagnostic confidence and helping avoid unnecessary anticoagulation.
MCQs:
Question 1
Which of the following statements regarding left ventricular thrombus assessment on cardiac imaging is MOST accurate?
A. Arterial phase imaging alone is sufficient to exclude left ventricular thrombus
B. Slow-flow artefact is most commonly seen in patients with normal ventricular function
C. Delayed phase imaging increases diagnostic confidence when evaluating intracavitary filling defects
D. True thrombus typically demonstrates progressive enhancement on delayed imaging
E. Cardiac MRI may demonstrate thrombus as an enhancing mass on late gadolinium imaging
Answer: C. Delayed phase imaging increases diagnostic confidence when evaluating intracavitary filling defects
Question 2
Which of the following is the most likely mechanism for the apparent apical filling defect seen on early phase CT imaging in this case?
A. Beam hardening artefact from coronary stents
B. Slow intracavitary contrast admixing due to regional wall motion abnormality
C. Acute embolic occlusion of the left anterior descending artery
D. Motion artefact from cardiac arrhythmia
E. Delayed myocardial enhancement from fibrosis
Answer: B. Slow intracavitary contrast admixing due to regional wall motion abnormality
Question 3
In patients with prior myocardial infarction and impaired left ventricular systolic function, left ventricular thrombus is clinically important primarily because it may lead to:
A. Ventricular free wall rupture
B. Coronary artery dissection
C. Systemic embolisation
D. Pulmonary hypertension
E. Constrictive pericarditis
Answer: C. Systemic embolisation
References:
- Radswiki T, Hacking C, Campos A, et al. Intracardiac thrombus. Reference article, Radiopaedia.org (Accessed on 12 Mar 2026) https://doi.org/10.53347/rID-12660
- Takaoka H, et al. Assessment of left ventricular thrombi using cardiac CT: A comparative evaluation of non-contrast, CT-angiography, delayed-enhanced images, and extracellular volume maps. J Cardiovasc Comput Tomogr. 2026 Jan-Feb;20(1):25-32. doi: 10.1016/j.jcct.2025.10.015. Epub 2025 Nov 10. PMID: 41219031.


