Click on the links below to view each section of the document and access the interactive maps.
- Foreword
- Acknowlegements
- Executive Summary
- Introduction
- CT scanner base in the UK
- CTCA delivery in the UK
- Projected requirement for CTCA following updated NICE CG95 guidelines
- Projected requirement for CTCA – absolute increase in provision needed
- Projected requirement for CTCA – relative increase in provision needed
- Specialist workforce
- Education and Training
- Abbreviations
- References
Available to members only:
Additional map – status of CT scanners around the UK
Foreword
The recently published National Institute for Health and Care Excellence (NICE) clinical guideline on ‘Chest pain of recent onset: assessment and diagnosis (CG95)’, suggests Computed Tomography Coronary Angiography (CTCA) as the rst line investigation for patients with stable chest pain if clinical assessment indicates typical or atypical angina, or non-anginal chest pain with ECG changes suggesting underlying coronary artery disease. Functional imaging or invasive angiography is recommended as a second-line investigation in those cases where CTCA is equivocal or positive i.
CTCA is a relatively new technique and therefore the number of professionals currently trained in its acquisition and reporting is limited. Also, high quality, low dose, CTCA also can only be performed using relatively modern CT equipment. For these reasons there is geographic variation in the availability and delivery of CTCA services within the UK.
Based on available data, the BSCI/BSCCT have assessed the current provision of CTCA
and modelled the expected demands on services, based on the current sustainability and transformation plan (STP) populations in England, and Health Boards in the devolved nations. This report, which we welcome, should prove helpful to commissioners of these services, to hospitals providing clinics for the assessment of those with suspected stable cardiac chest pain, and to those considering the workforce implications of providing CTCA services more widely and to national standards ii.
Professor Huon Gray
National Clinical Director for Heart Disease, NHS England
Dr Nicola Strickland
President, Royal College of Radiologists
Acknowledgements
Thanks to our industry partners for providing the commercial data on the CT scanner base, colleagues in NHS England and devolved Nations for activity data, and the staff of BSCI/ BSCCT and SCCT for accreditation data. Thanks to Dr John Driesbach for data ordering & cleansing and Dr Giles Roditi for data analysis & production of the maps within this document.
The BSCI/BSCCT has worked hard to ensure the veracity of the data within this report. Nonetheless it should be acknowledged that data on volumes of CTCA speci cally are challenging due to the quality of, and potential variety of, coding data held centrally. Determining exact gures for RACPC attendance in the UK has been extrapolated from
the English data used by NICE, whilst the process for estimating the potential upper limit of stable chest pain referrals, to whom the NICE CG95 update applies, from all sources, has also required extrapolation from historic peer reviewed publications.
Authors:
Dr Ed Nicol
President, British Society of Cardiovascular Imaging and British Society of Cardiovascular CT (BSCI/BSCCT)
Dr Simon Padley
Lead for Accreditation BSCI/BSCCT
Dr Giles Roditi
President-Elect BSCI/BSCCT
Professor Carl Roobottom
Lead for Research BSCI/BSCCT
Executive Summary
There has been a sustained growth in the provision of cardiovascular CT, including CTCA, in the UK since that described in 2010 iii, however the delivery of CTCA remains highly variable across the UK and even within regions. The introduction of the new NICE guidelines for stable chest pain will require signi cant investment in new technology, a far wider and more uniform geographical delivery of CTCA, and extensive investment in the clinical workforce to ensure training and experience is accessible and provided, to deliver high quality CTCA against agreed standards ii. This paper focusses speci cally on the location of cardiac capable scanners (whether cardiac enabled or not), the location and number of individuals currently accredited in cardiovascular CT and the current delivery of CTCA both by centre and population.
To ensure the quality of CTCA provision remains high in the UK it will be necessary to ensure that:
- CTCA is performed on appropriate, cardiac enabled, CT scanners with adequate reporting workstation software to allow thorough and complete analysis and report generation.
- The workforce (radiographers, nurses, radiologists and cardiologists) are appropriately trained in CTCA and are both con dent and competent to acquire CTCA images in all patients, including those who may be technically challenging (high heart rates, arrhythmias, high BMI etc.).
- Departments develop close relationships with local centres of excellence (and level 3 accredited practitioners) and industry partners to ensure an ongoing, iterative process to protocol optimisation.
- Departments have appropriate medical physics support to routinely assess the doses delivered for CTCA locally and ensure that they are close to the National Dose Reference Level (NDRL)*
* A NDRL is expected to be published by Public Health England in early 2017. This will be based on the results of the BSCI/BSCCT National dose survey iv with a median dose for CTCA of 200mGy.cm.
Introduction
CT coronary angiography (CTCA) is a non-invasive, x-ray based, technique that allows assessment of both the coronary artery lumen as well as atheromatous plaque morphology. CTCA has almost 100% accuracy in excluding functionally significant (chest pain producing) coronary artery disease and can help detect those at high risk of developing acute coronary syndromes v.
Whilst current doses for CTCA in the UK are acceptable (median 200mGy.cm) iv, it is a demanding radiological technique, that requires a thorough understanding of ECG-gated protocols, dose optimisation strategies and CT scanner technology. Without specific training of both radiographers and medical practitioners, CTCA can be a high-dose technique delivering sub-optimal image quality.
Specific standards for the acquisition of CTCA have been published by the BSCI/BSCCT
and endorsed by both the Royal College of Radiologists and Royal College of Physicians ii. Additional guidelines on appropriate scanner technology for cardiovascular CT has been published by NICE vi.
CTCA has almost 100% accuracy in excluding significant coronary artery disease (CAD) and when compared with functional imaging tests or invasive angiography it is the lowest cost technique. The rapid technological advances that allow CTCA to be delivered at a low dose and the substantial amount of new scientific evidence published support its widespread use in clinical practice vii viii ix and provide the backdrop to the recent NICE review. The review of the evidence has brought about the new recommendations that propose CTCA as the most clinically and cost effective diagnostic first line test for all patients presenting with stable chest pain.
The new guidelines present considerable delivery challenges in the short term. CTCA is a relatively new technique and therefore the number of professionals trained in its acquisition and reporting are limited, with considerable geographic variation in delivery and practice within the UK. High quality, low dose, CTCA also can only be performed on relatively modern CT equipment.
To assess the current provision and capability within the UK the BSCI/BSCCT has worked closely with industry partners, the Royal College of Radiologists, British Cardiovascular Society, and other national stakeholders to obtain detailed and accurate data on current UK cardiovascular CT (including CTCA) practice. The BSCCT has looked at infrastructure (including equipment), current delivery of CTCA and cardiovascular CT services, and accredited personnel figures to assess the likely impact of the updated NICE guidelines in the delivery of the requirements proposed for assessment of patients with stable chest pain. We have also modelled the expected demands on these services, based on the current sustainability and transformation plan (STP) populations in England and Health Boards in the devolved nations to produce Red-Amber-Green (RAG) maps that visually highlight the key areas that need addressing.
CT Scanner Base in the UK
The UK has some of the most intensively used MRI and CT scanners in the EU x and the demand for general CT continues to grow in the UK. In the last decade CT studies performed have risen by 160% whilst between 2012 and 2015 demand increased 29% in England and 55% in Scotland xi. Even for general CT there is currently a lack of capacity to respond to this demand. The UK has a very low number of CT scanners as compared with other OECD countries, with around 9 CT scanners per million population; compared to Germany (19), Spain (17), and France (14) per million population xii.
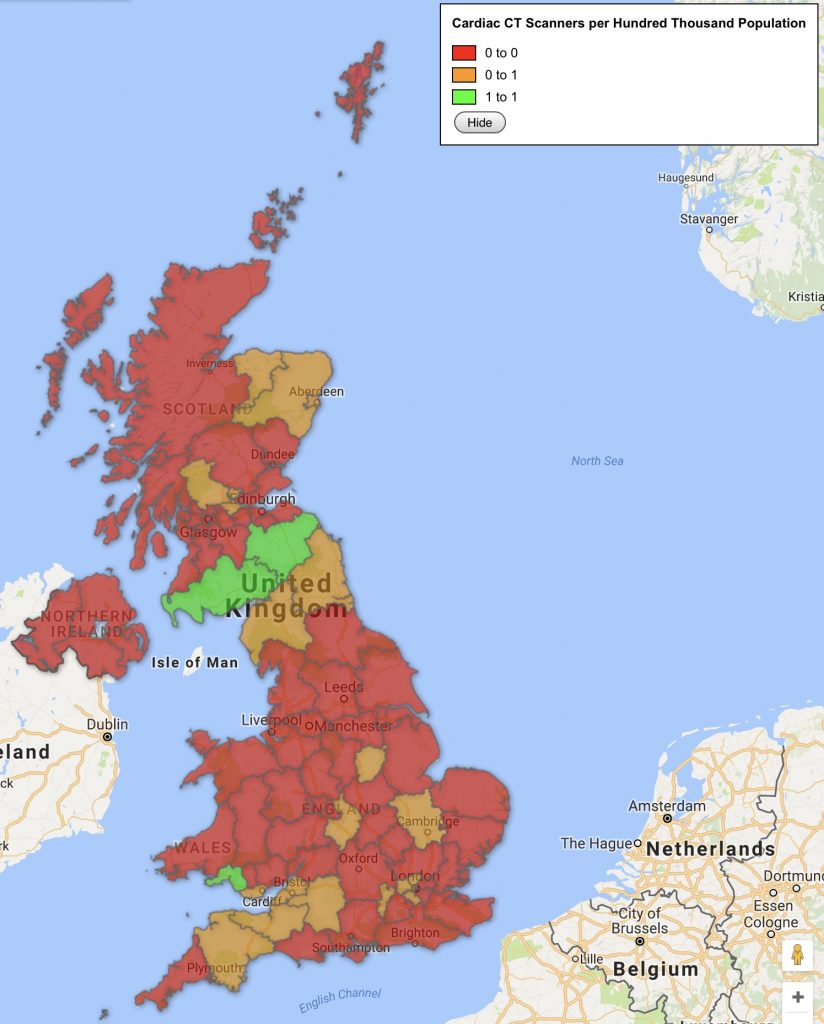
Map 1. Cardiac enabled scanners by region in the UK*
As per NICE guidelines, Cardiac CT scanners must be of a higher specification; they must be a minimum of 64-detector technology, however, as NICE have previously commented, both dose and image quality are better on more modern technology vi.
The BSCI/BSCCT, working with all the CT manufacturers, has created a database of cardiac capable CT scanners. Currently there are only 228 cardiac capable scanners in the UK (this equates to 4 scanners/million patients and 50% of all CT scanners in the UK) with wide geographic variation (see Map 1).
Not all are cardiac enabled (i.e. they do not have the required software to support CTCA acquisition). Therefore, the additional workload that will be generated by the new NICE guidelines will require investment in both hardware (cardiac enabled CT scanners) and software (to allow these scanners to be used to acquire, and generate CTCA studies).
* STP in England, Regional Health Boards in Scotland, Northern Ireland and Wales
CTCA Delivery in the UK
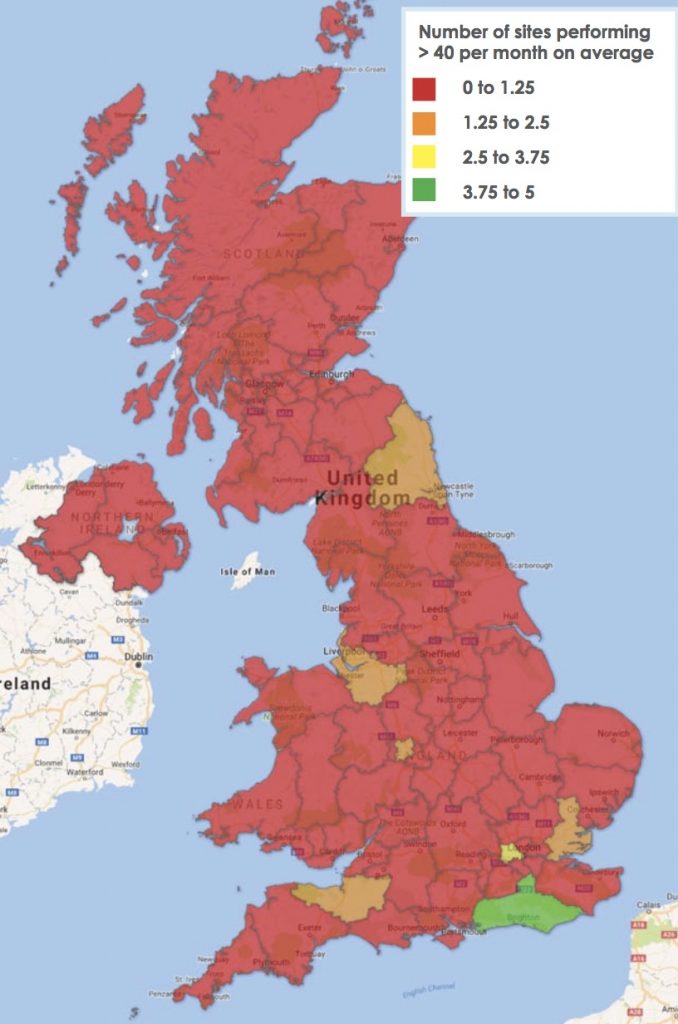
The BSCI/BSCCT has obtained national data for the current provision of cardiovascular CT for 2015 (Map 2). This data demonstrates the low number of centres performing high volumes within each region.
Map 2. Number of centres per region* performing >40 CTCA per month
101 centres performed a total of 38,455 ECG-gated cardiac CT scans** (including CTCA) in the UK in 2015. 34% of these scans are performed in the 10 largest centres in the UK. 68% of centres who undertake Cardiovascular CT perform <10 cardiac scans per week. Of the Trusts that deliver Cardiovascular CT currently <10% perform >40 scans per month.
In Scotland 8 centres are currently performing cardiac CT in Scotland with only one centre performing > 10 cardiovascular CT scans per week.
There are 7 cardiovascular CT centres in Wales and 5 in Northern Ireland Only one Welsh centre performs >10 cardiovascular CT scans per week with no higher volume centres in Northern Ireland.
* STP in England, Regional Health Boards in Scotland, Northern Ireland and Wales
** Cardiac CT coded CACRY
Projected requirement for CTCA following updated NICE GG95 guidelines
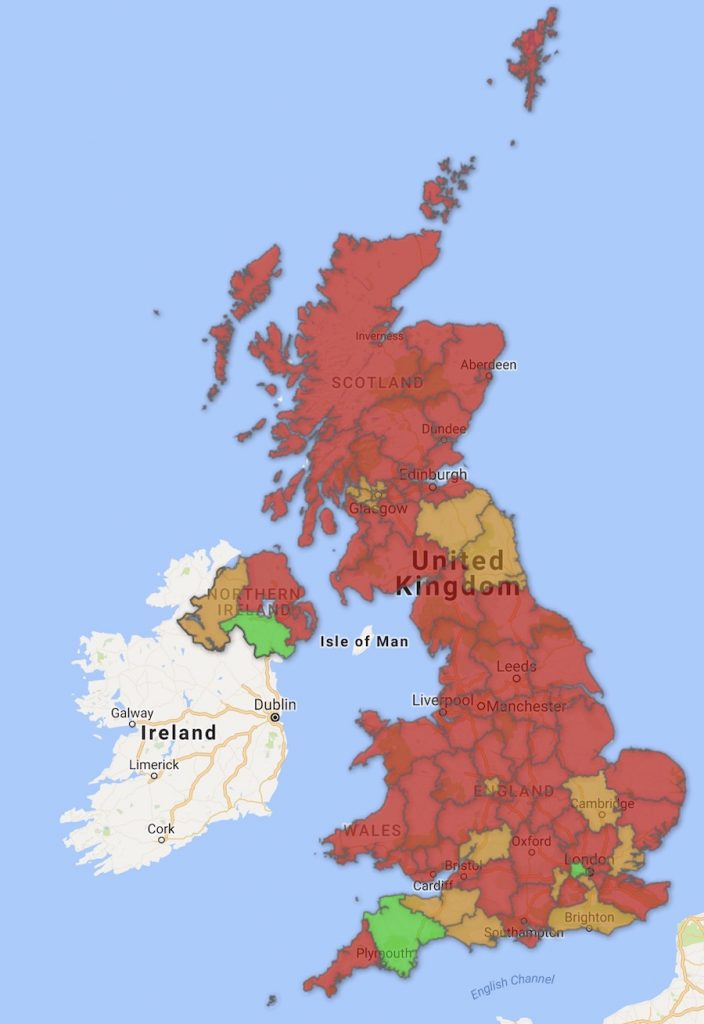
In 2010 there were 120,000 referrals to rapid access chest pain clinics (RACPC) in England i. This would equate to 148,000 referrals per year in the UK (assuming an equivalent attendance to RACPC in Wales, Scotland and NI). This equates to 200 CTCA per 100,000 population, if 90% were referred for CTCA. Currently only 2 regions in the UK (Devon and North West London) are currently delivering this volume of CTCA.
Map 3. CTCA per 100,000 population by region* in the UK
However, as not all patients with chest pain go through a RACPC, this number is likely to represent an underestimation of the total referrals generated for CTCA. Patients also present via the emergency department (ED), medical admissions units (MAU) and via specialty clinics.
Using previous published assumptions used to predict the demand in nuclear cardiology for myocardial perfusion scintigraphy (MPS) xiv the true gure may be as high as 340,000 referrals per annum (or 523 CTCA per 100,000 population, per annum).
It is therefore estimated that up to an additional 200,000 patients may require CTCA under the new NICE stable chest pain guidelines. This represents a 700% increase in cardiovascular CT delivery.
Projected Requirement for CTCA – Absolute Increase in Provision Needed
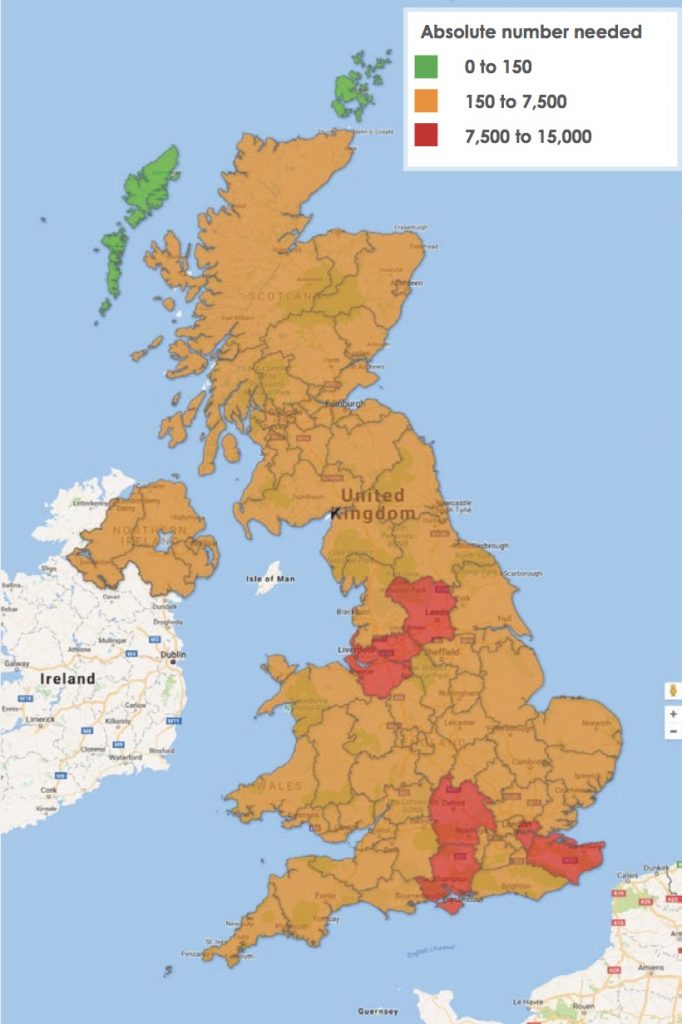
Map 4. Absolute increase in number of CTCA required by region* in the UK
Conversely, in more heavily populated regions, such as Greater Manchester, there is also a relatively low provision to the large population and nearly 15,000 extra scans will be required per year to meet the projected NICE guidelines. This represents a 7000% increase compared with current activity. Even in North-West London where CTCA activity is to be highest in the UK, the proportionate increase in activity is the lowest but still requires a 100% increase in throughput. This is not an insigni cant change in delivery for any cardiac CT service.
* STP in England, Regional Health Boards in Scotland, Northern Ireland and Wales
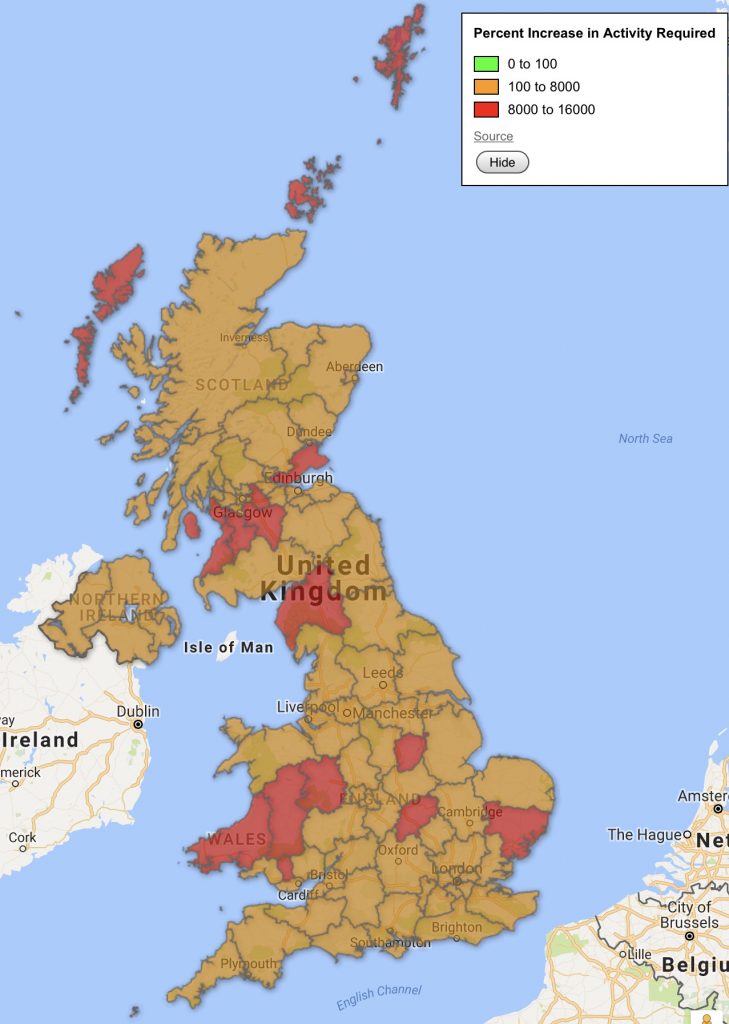
Projected Requirement for CTCA – Relative Increase in Provision Needed
Map 5. Percentage increase in number of CTCA required by region* in the UK
It is clear that the UK cardiovascular CT community faces a significant challenge to deliver the output required from this revision to NICE guidance. Even the best prepared regions and departments face a minimum of a doubling of CTCA scans they are asked to provide.
Many centres will face much greater increases in demand, and some will effectively be starting from scratch. It must also be understood that the revised guidelines come with no additional funding, and for many centres the recommended numbers will remain aspirational for some time.
* STP in England, Regional Health Boards in Scotland, Northern Ireland and Wales
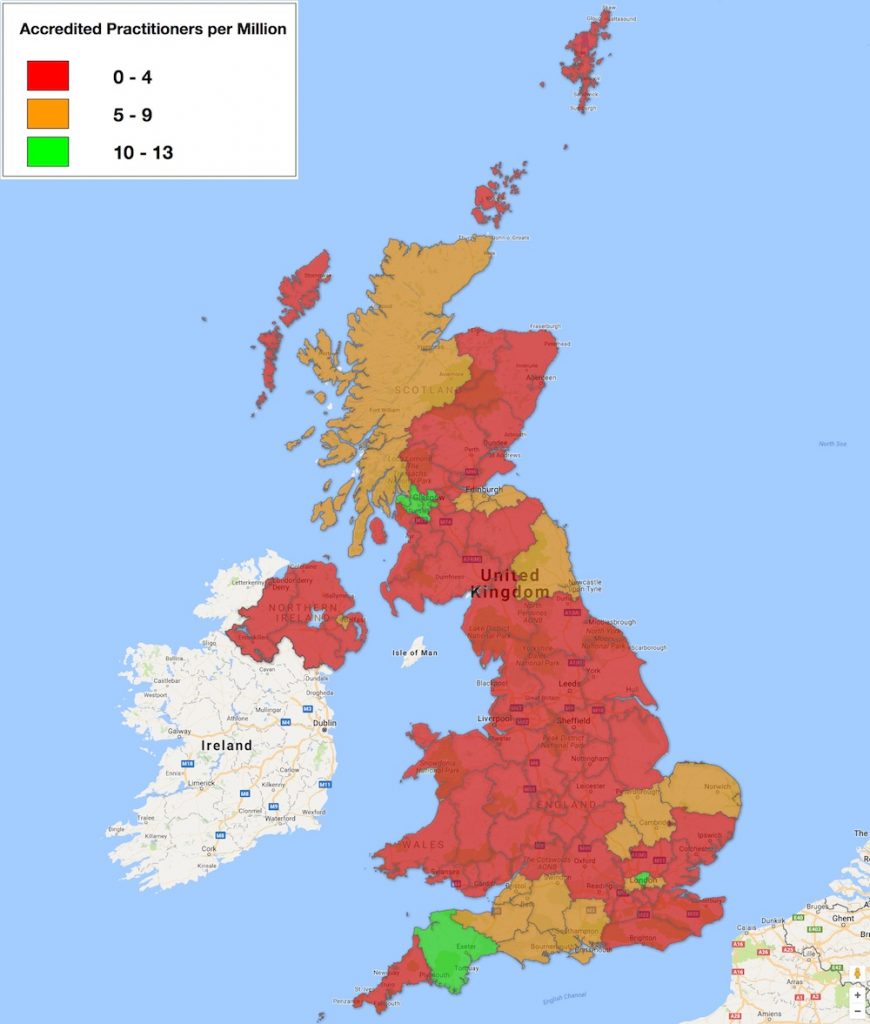
Specialist workforce
CTCA scans require expertise to acquire and report. In the UK CTCA reporting is usually done by Radiologists and/or Cardiologists. However, the number of available specialists is low.
Map 6. Accredited CTCA Practioners by region* in the UK
There is a general shortage of Radiologists in the UK with a recent Royal College of Radiologists (RCR) report demonstrating that the UK has a low number of radiologists compared to our European counterparts. The UK has 48 radiologists per million population compared with Germany (92), Spain (112) and France (130) xv. As a result of activity growth outstripping workforce growth, imaging departments are struggling to keep up with demand. In 2015, 99% of departments were unable to meet their general radiology reporting requirements.
Detailed information of all medical practitioners who have obtained accreditation to report CTCA (either through the BSCI/BSCCT or SCCT) has been collated and whilst accreditation is not currently a requirement to practice, it is a proxy marker of good medical practice, and as such is used for revalidation purposes. Map 4 demonstrates the number of accredited practitioners (Level 2 accreditation) in the UK is relatively small and there is significant regional variability.
* STP in England, Regional Health Boards in Scotland, Northern Ireland and Wales
Education and Training
Accreditation in cardiovascular CT can be achieved via both the BSCI/BSCCT and the SCCT. Level 2 accreditation indicates competence to report whilst level 3 indicates a level of experience to train others in CTCA.
Map 7. Level 2 (red dots) and Level 3 (blue pins) accredited CTCA practitioners in the UK.
To deliver a high quality CTCA service across the UK will require signi cant investment in training. The whole workforce (radiographers, nurses, medical physicists, radiologists and cardiologists) will need to be appropriately trained in both the clinical and technical aspects of CTCA so they are both confident and competent to acquire CTCA images in all patients, including those who may be technically challenging (high heart rates, arrhythmias, high BMI etc.). This will also ensure that Quality Assurance is delivered as a key component of a high quality CTCA service xvi.
Whilst core and advanced education in CTCA is provided by both the BSCI/ BSCCT and individual providers, it will be necessary to significantly expand these educational offerings and look at alternative methods of delivery. This will require concerted and co-ordinated effort by those responsible for the clinical and technical education of the workforce, in conjunction with the specialist societies to ensure that high quality CTCA is delivered at optimal (as low as reasonably achievable) radiation doses.
* STP in England, Regional Health Boards in Scotland, Northern Ireland and Wales

Abbreviations
- BMI Body Mass Index
- BSCI/BSCCT British Society of Cardiovascular Imaging / British Society of Cardiovascular Computed Tomography
- CT Computed Tomography
- CTCA Computed Tomography Coronary Angiography
- ED Emergency Deprtment
- MRI Magnetic resonance Imaging
- NDRL National Dose Reference Level
- NICE National Institute of Health & Care Excellence
- OECD Organisation for Economic Co-operation and Development RACPC Rapid Access Chest Pain Clinic
- RAG Red Amber Green
- RCP Royal College of Physicians
- RCR Royal College of Radiologists
- SCCT Society of Cardiovascular Computed Tomography
- STP Sustainability & Transformation Plan
- UK United Kingdom
References
- National Institute of Healthcare Excellence (NICE) clinical guidelines on Chest pain of recent onset: assessment and diagnosis (CG95)
- Harden SP, Bull RK, Bury RW, Castellano EA, Clayton B, Hamilton MC, Morgan-Hughes GJ, O’Regan D, Padley SP, Roditi GH, Roobottom CA, Stirrup J, Nicol ED; The safe practice of CT coronary angiography in adult patients in UK imaging departments. CTCA standards working party of the British Society of Cardiovascular Imaging, the Royal College of Physicians and the Royal College of Radiologists. Clin Radiol. 2016 Aug;71(8):722-8. doi: 10.1016/j.crad.2016.04.008. Epub 2016 May 17.
- Mittal T, Nicol E, Harden S, Roobottom, C, Padley S, Roditi G, Peebles C, Taylor A, Hamilton M, Morgan-Hugs G, Bury R. On behalf of the British Society of Cardiovascular Imaging (BSCI) The national evolution of cardiovascular CT practice: A UK NHS perspective. Int J Cardiol. 2013 Apr 29. doi:pii: S0167-5273(13)00589-5.10.1016/j.ijcard.2013.04.005
- Nicol E, Castellano I, Harden S. A National Survey of Coronary CT Angiography Doses in the UK (on behalf of the British Society of Cardiovascular CT (BSCCT). Journal of Cardiovascular CT 2016:S60
- Maurovich-Horvat P, Ferencik M, Voros S, Merkely B, Hoffmann U. Comprehensive plaque assessment by coronary CT angiography. Nat Rev Cardiol. 2014 Jul;11(7):390-402. doi: 10.1038/nrcardio.2014.60
- https://www.nice.org.uk/guidance/dg3
- Douglas PS, Hoffmann U, Patel MR, Mark DB, Al-Khalidi HR, Cavanaugh B, Cole J, Dolor RJ, Fordyce CB, Huang M, Khan MA, Kosinski AS, Krucoff MW, Malhotra V, Picard MH, Udelson JE, Velazquez EJ, Yow E, Cooper LS, Lee KL; PROMISE Investigators. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med. 2015 Apr 2;372(14):1291-300. doi: 10.1056/NEJMoa1415516.
- SCOT-HEART investigators. CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. 2015 Jun 13;385(9985):2383-91. doi: 10.1016/S0140-6736(15)60291-4. Erratum in: Lancet. 2015 Jun 13;385(9985):2354.
- Williams, Michelle C, Amanda Hunter, Anoop S V Shah, Valentina Assi, Stephanie Lewis, Joel Smith, Colin Berry, and others. “Use of Coronary Computed Tomographic Angiography to Guide Management of Patients with Coronary Disease.” Journal of the American College of Cardiology 67, no. 15 (2016): doi:10.1016/j. jacc.2016.02.026.
- Cylus J, Richardson E, Findley L et al. United Kingdom: health system review. Health Syst Transit 2015;17:1–125
- https://www.rcr.ac.uk/clinical-radiology/service-delivery/rcr-workforce-census
- https://www.oecd.org/els/health-statistics-2014-frequently-requested-data.htm
- http://webarchive.nationalarchives.gov.uk/20130107105354/http:/www.dh.gov.uk/en/Publicationsandstatistics/Statistics/Performancedataandstatistics/Integratedperfomancemeasuresmonitoring/DH_112551
- Underwood SR, Anagnostopoulos Cerqueira C, Ell PJ, Flint EJ, Harbinson M, Kelion AD, Al-Mohammad A, Prvulovich AP, Shaw LJ, Tweddel AC. Myocardial perfusion scintigraphy: the evidence. A consensus conference organised by the British Cardiac Society, the British Nuclear Cardiology Society and the British Nuclear Medicine Society, endorsed by the Royal College of Physicians of London and the Royal College of Radiologists. European Journal of Nuclear Medicine and Molecular Imaging 2003:31(2);261-291
- Royal College of Radiologists, How the next Government can improve diagnosis and outcomes for patients: Four proposals from the Royal College of Radiologists. 2015.
- White S, Castellano I, Gartland N, Patel T, Padley SP, Rubens MB, Nicol E. Quality Assurance in Cardiovascular CT: A Practical Guide. Clin Rad 2016 Aug;71(8):729-38. doi: 10.1016/j.crad.2016.01.024. Review.


