By Dr Katharine Garfath-Cox
University of Southampton
A 30 year old male presented to the emergency department with atypical chest pain and a mildly elevated troponin. He was referred for a CT coronary angiogram to exclude coronary artery disease.
The CTCA was acquired using a tight bolus of contrast and a region of interest in the ascending and descending aorta to enable maximal contrast density within the coronary arteries. The coronary arteries were normal. The scan demonstrated near equal contrast density within the right and left heart chambers and a significantly dilated right atrium and right ventricle.
A systematic review was employed to discover the site of the presumed left to right shunt. A sinus venosus ASD (figure 1a) was present with associated anomalous drainage of the right superior pulmonary vein (figure 1b,1e,1f).
Discussion:
Atrial septal defects are the most common congenital cardiac anomaly detected in adult patients (1)(2). There are four main types, Ostium Primum, Ostium Secundum, Sinus Venosus Defect and coronary sinus type. The sinus venosus defect occurs in only approximately 5% of cases and these defects are present at the entrance of the SVC and are associated with a partial anomalous pulmonary venous connection (PAPVC).
The clinical presentation may be delayed due to low atrial pressures and even large defects can be well tolerated. The haemodynamic consequence of the defect results in a dilated right atrium and right ventricle with an increase in pulmonary vascularity. The other cardiac chambers remain normal in size.
Diagnosis is often achieved with Echo, however, with an increasing number of CT coronary angiograms being performed, review of cardiac chambers and anomalous connections is essential. The advantage of CT in this case over Echo is the concurrent identification of the site of the PAPVC, important for surgical planning.
Figure legend:
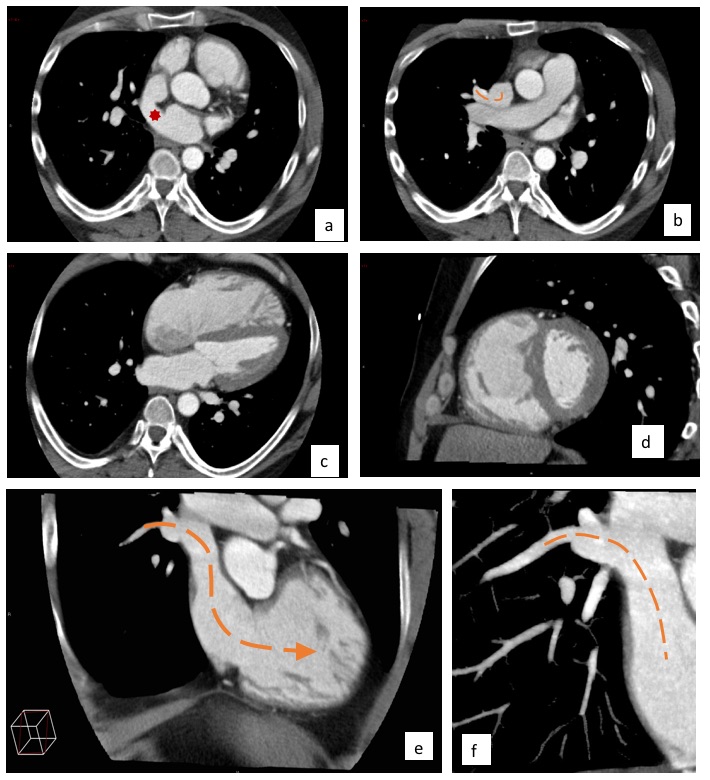
Figure1. Single beat, 16cm detector CTCA.
1a. Axial image showing a large sinus venosus ASD at the level of the entrance of the SVC into the RA (red star).
1b. Axial image of the superior pulmonary vein draining into the lateral aspect of the SVC.
1c. 4 chamber view of the dilated right atrium and right ventricle.
1d. 2 chamber view of the dilated right atrium and right ventricle.
1e. Coronal reformatted image showing the PAPVC.
1f. Cropped coronal reformat of the PAPVC.
Multiple choice questions
1. Which is the most common type of ASD?
A) Ostium primum ASD
B) Superior sinus venosus defect
C) Inferior sinus venosus defect
D) Unroofed coronary sinus type
E) Ostium Secundum ASD
2. What are the haemodynamics of an ASD?
| Right atrium | Right ventricle | Left atrium | Left ventricle | Pulmonary vasculature | Aorta | |
| A | Dilated | Dilated | Unchanged | Unchanged | Increasde | Normal |
| B | Unchanged | Dilated | Unchanged | Unchanged | Decreased | Normal |
| C | Dilated | Dilated | Unchanged | Unchanged | Normal | Normal |
| D | Normal | Normal | Dilated | Dilated | Increased | Enlarged |
| E | Dilated | Dilated | Dilated | Unchanged | Increased | Normal |
3. This patient re-presents to the emergency department prior to intervention with breathlessness and mild cyanosis. Reversal of the shunt is identified on echocardiogram and a diagnosis of Eisenmenger physiology is made. What finding would be a feature on imaging due to the resultant pulmonary arterial hypertension?
A) Dilated pulmonary veins
B) Small central pulmonary artery
C) Mural calcification in main pulmonary arteries
D) Mural calcification in main pulmonary veins
E) Mural calcification in peripheral pulmonary arteries
4. Which of the following statements is not true regarding PAPVC?
A) Scimitar syndrome is a type of PAPVC
B) Common connections can be classified as supra-cardiac, cardiac or infra-cardiac.
C) 15% have an associated ASD
D) All pulmonary veins drain into the systemic circulation.
E) PAPVC is not always cyanotic
Images with thanks to Dr Russell Bull, Royal Bournemouth Hospital.
Answers
(1 E), (2 A, B= Tetralogy of Fallot , C=Ebstein anomaly, D=PDA), (3 C), (4 D)


