Author
Dr Salma Selim 1, Dr Matthew Morgan1, Dr Abbas Ausami1
1 University Hospital Southampton NHS Foundation Trust.
Case history
A 65-year-old lady presented to A&E with central chest pain, nausea and clamminess. Serial troponins were raised at 175 and 1124. ECG showed dynamic anterior wall change. The patient had a background of gastroesophageal reflux disease, limited systemic sclerosis. She had a previous diagnosis of Takotsubo cardiomyopathy in 2019. Initial bedside cardiac TTE demonstrated global hypokinesia sparing basal segments of the ventricles with ejection fraction between 5 to 10%.
CT coronary angiogram demonstrated circumferential dilatation of the mid-to-apical left ventricular cavity.
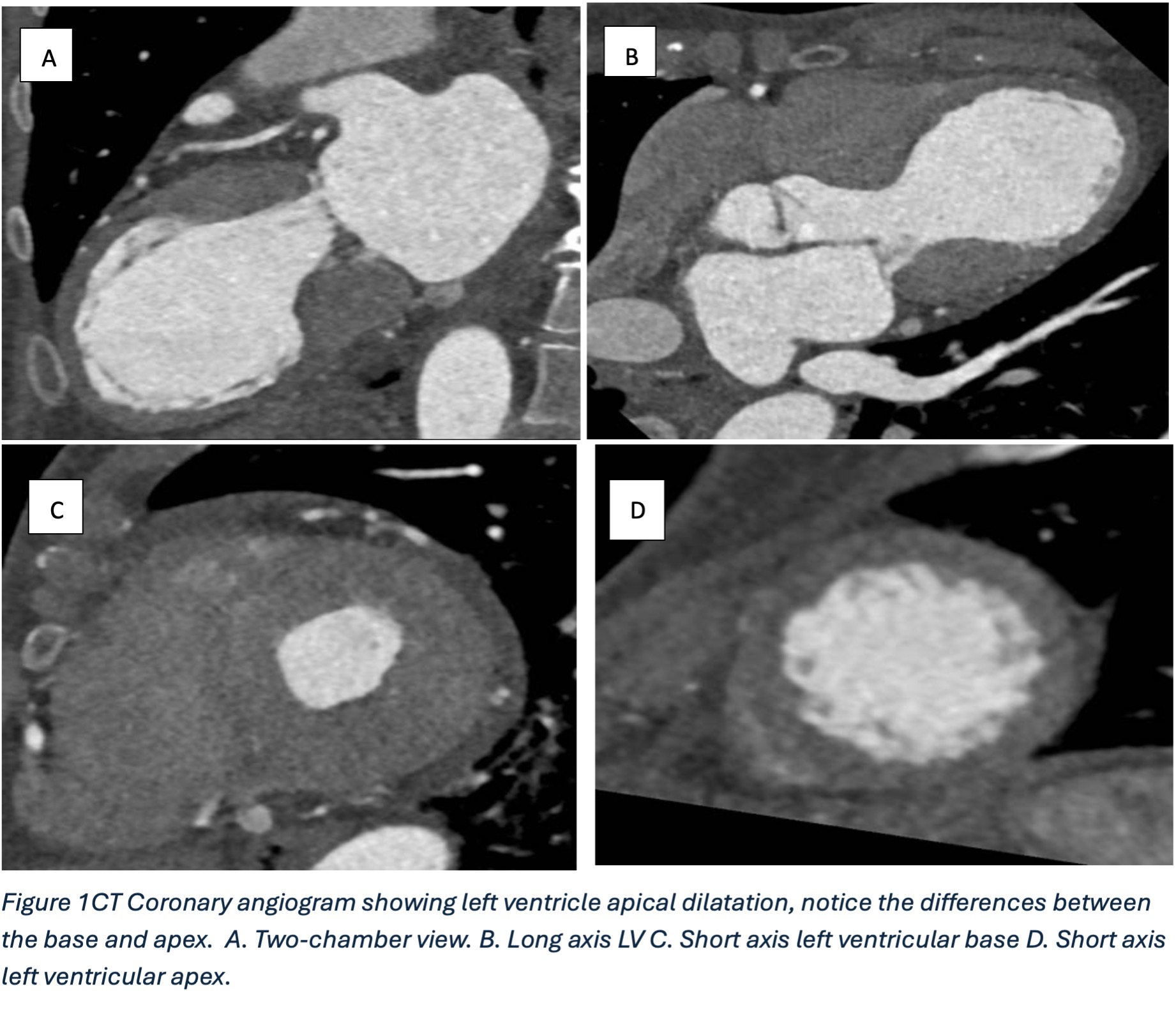
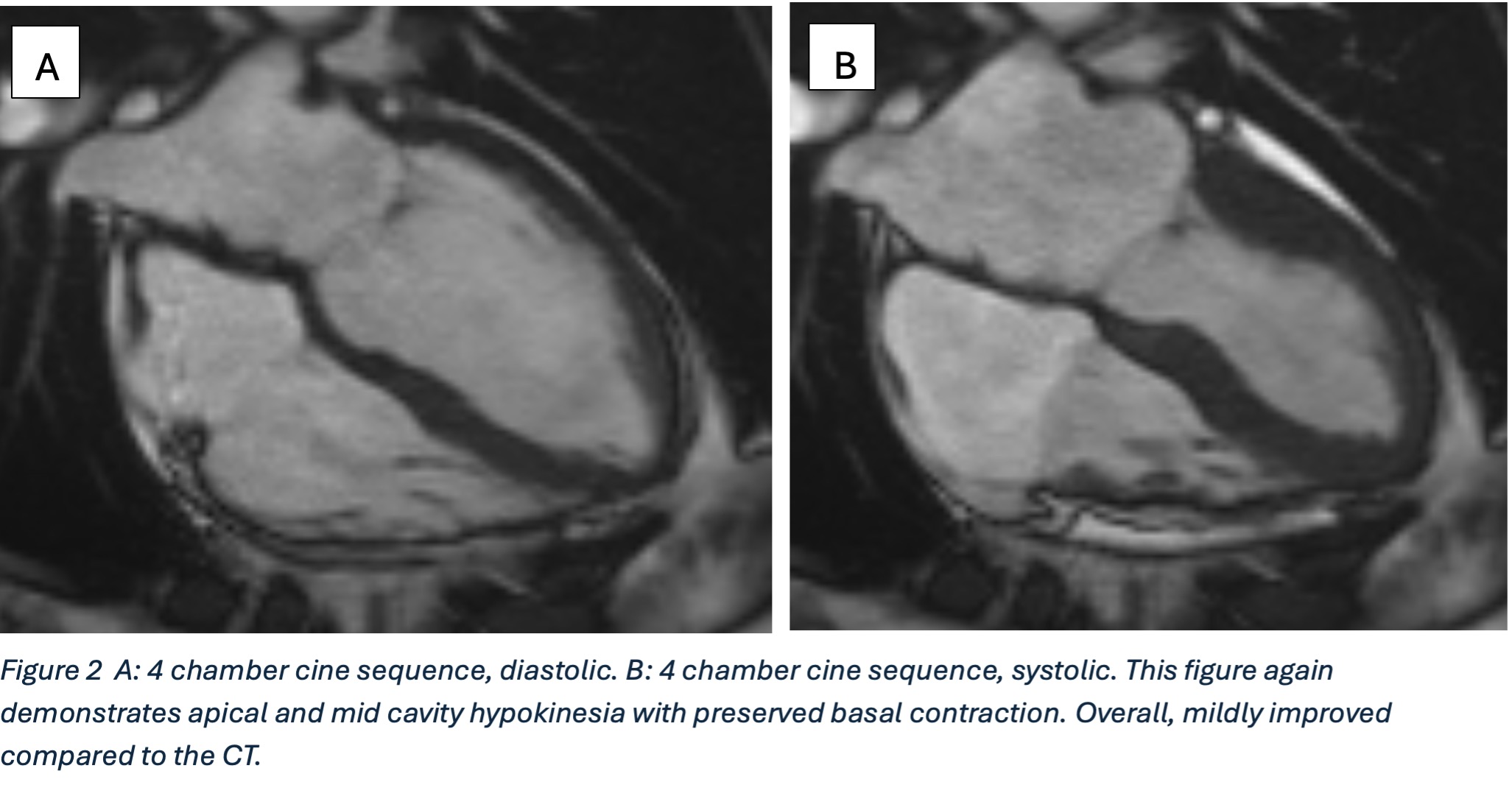
Cardiac MRI demonstrated mildly impaired resting systolic function and circumferential hypokinesis of the mid-to-distal left ventricular myocardium. Cine images demonstrated good contraction within the basal myocardial segments. The LV was not visually dilated.
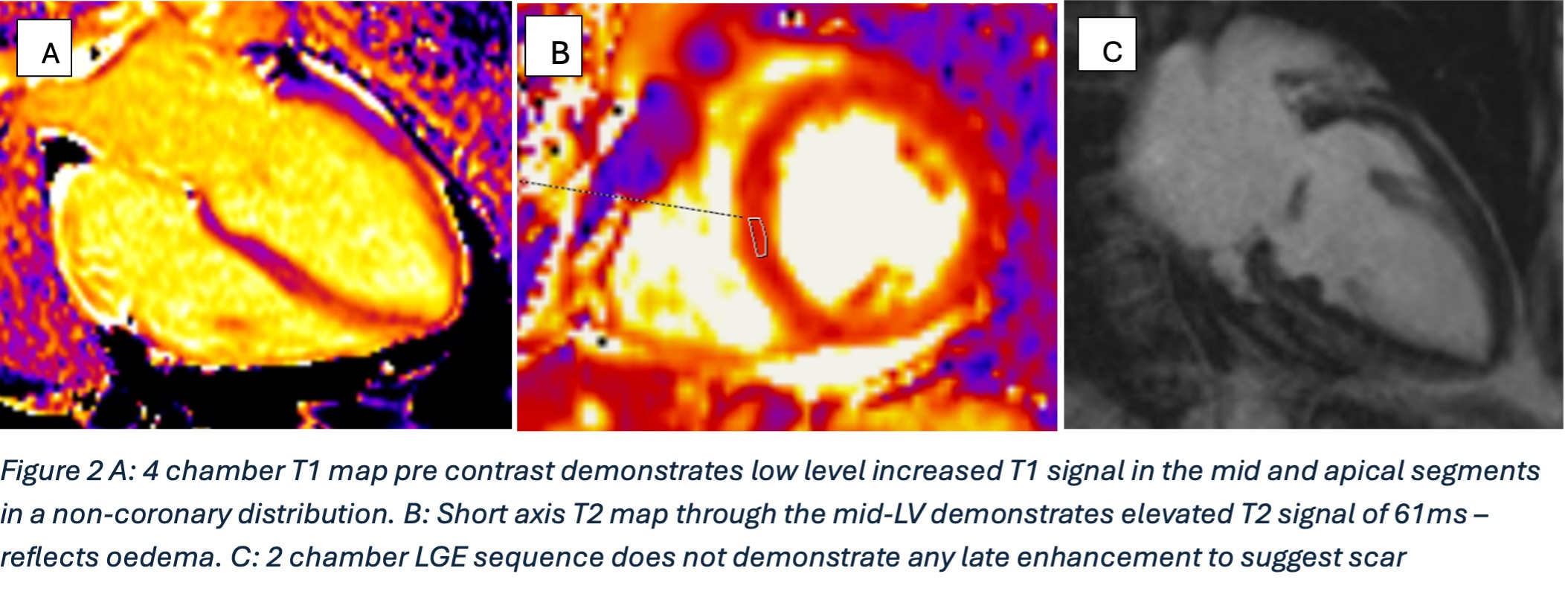
T1 mapping sequences demonstrated normal basal segment mapping times and elevated mid-distal segment mapping times. T2 images showed mid-to distal myocardial oedema and elevated T2 mapping times.
No late Gadolinium enhancement appreciated.
Questions
What is the Echocardiographic finding that is most characteristic of Takotsubo cardiomyopathy?
- Concentric LV Hypertrophy
- Regional Wall motion abnormality in a single coronary territory.
- Global hypokinesia.
- Apical ballooning with preserved basal contraction.
- Right ventricular dilatation.
Which is NOT a recognised complication of Takotsubo cardiomyopathy?
- Infarct
- Congestive Heart failure
- LV Rupture
- Stroke
- Pericarditis
What is the most common demographic affected by Takotsubo cardiomyopathy?
- Young male athletes
- Middle aged men with diabetes
- Post menopausal women after emotional stress
- Children under the age of 4
- Pregnant women in first trimester
(Answers:d,e,c)
Discussion
Symptoms of Takotsubo Cardiomyopathy are similar to acute coronary syndrome. Similarities between both conditions in symptoms, ECG Changes, blood biomarkers raise difficulty distinguishing between both for clinicians. Invasive angiography typically reveals apical ballooning of the left ventricle alongside patent coronary arteries. 1
In this case, given the patient’s previous diagnosis with Takotsubo cardiomyopathy and a bedside echocardiogram showing global hypokinesia sparing the basal segment, a CT coronary angiogram was performed instead followed by a cardiac MRI. The lack of late gadolinium enhancement adds diagnostic confidence, since takotsubo remains a diagnosis of exclusion 1
A fundamental characteristic of takotsubo is the spontaneous recovery of the LV ejection fraction, normalises in nearly all patients over a variable period (days to weeks). However, there is a recognised early mortality of 3-5% due to arrythmias, pump failure, cardiac rupture or thromboembolic complications. There is a recognised recurrence rate, of 10%–15%, where the trigger and phenotype is typically different and the interval of time to a recurrence is unpredictable.1 In this case, the patient did not report a specific stressful event that may have triggered this episode.
On cardiac MRI, four patterns have been described: apical (most common), biventricular, mid-ventricular, and basal. Absence of bright late gadolinium enhancement and vascular territory distribution helps differentiate Takotsubo cardiomyopathy from MI. There can be a mildly increased T2 intensity signal due to myocardial oedema which typically involves the affected segments.2 Evidence of transient left ventricular dysfunction with apical “ballooning” or dyskinesis involving more than one discrete coronary artery territory is recognised as one of the diagnostic criteria for Takotsubo cardiomyopathy.3
Reference:
1 Dawson DK. Acute stress-induced (takotsubo) cardiomyopathy. Heart 2018;104:96-102. https://doi.org/10.1136/heartjnl-2017-311579
2 Weerakkody Y, Campos A, Sharma R, et al. Takotsubo cardiomyopathy. Reference article, Radiopaedia.org (Accessed on 18 May 2025) https://doi.org/10.53347/rID-25099
3 Carroll D, Campos A, Rasuli B, Takotsubo cardiomyopathy (diagnostic criteria). Reference article, Radiopaedia.org https://doi.org/10.53347/rID-94359


