Submitted by Dr Carina Brolund-Napier (CT2 Core Medical Trainee), Dr Amit Parekh (Radiology SPR), Dr Rajiv Singh (Consultant Radiologist,), Dr Garrett McGann (Consultant Radiologist). Gloucestershire Hospitals NHS Foundation Trust, UK.
A 65 year old man presented with atypical chest discomfort and dyspnoea on a background of hypertension, hypercholesterolaemia and a positive family history of coronary artery disease. Coronary angiography showed diffuse calcific atheroma, ectatic arteries, a coronary aneurysm and a coronary-pulmonary fistula. Further imaging with computed tomography (CT) coronary angiography identified a complex fistula between a branch of the proximal left anterior descending artery feeding into a 31mm x 33mm aneurysmal segment around the right ventricular outflow tract (RVOT), in turn fistulating with the pulmonary trunk. There was also a collateral network of dilated tortuous vessels seen anastomosing around the RVOT in keeping with a Vieussens arterial ring, a collateral pathway between the right and left coronary arteries. There was no demonstration of ischaemia on stress MRI.
Seven years later, the patient was re-referred to cardiology with intermittent atypical chest discomfort. A repeat cardiac CT showed the aneurysm had increased in size to 51mm x 55mm with possible thrombus formation. The case was discussed at the cardiothoracic MDT where the consensus of opinion was that due to the risk of rupture this would likely require surgical repair. Further imaging with coronary angiography was recommended to ascertain if coronary intervention would be necessary at the time of surgery.
Figure 1: Imaging at first presentation
1a – Three-dimensional reconstruction CT coronary angiography. A network of dilated tortuous collateral coronary vessels with a 31mm x 33mm aneurysm lying between the circumflex and left main stem.
1b – Axial image from CT coronary angiography demonstrating the left coronary artery feeding into the coronary aneurysm.
1c – Axial image from CT coronary angiography demonstrating an aneurysmal coronary artery fistulating into the pulmonary trunk (white arrow)
1d – Axial image from CT coronary angiography demonstrating a network of dilated tortuous vessels overlying the pulmonary trunk.
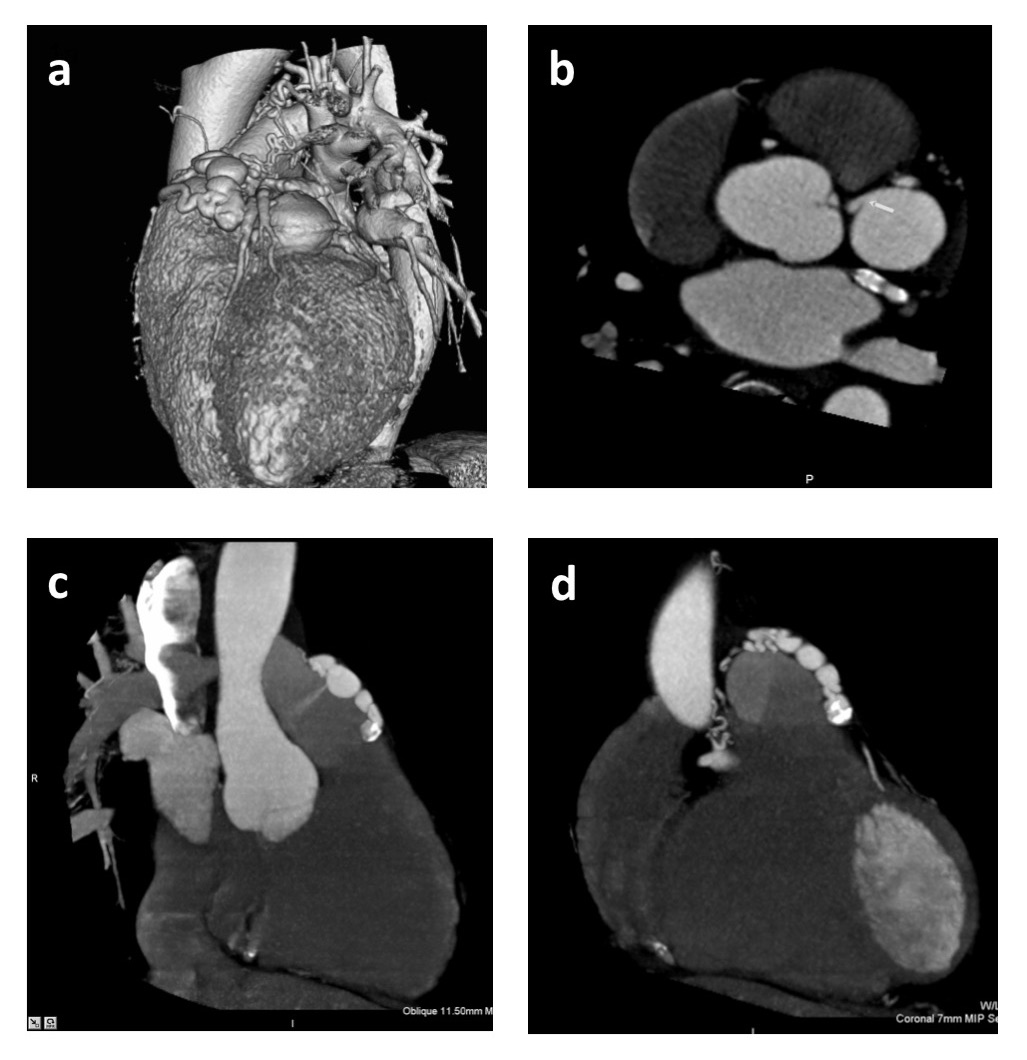
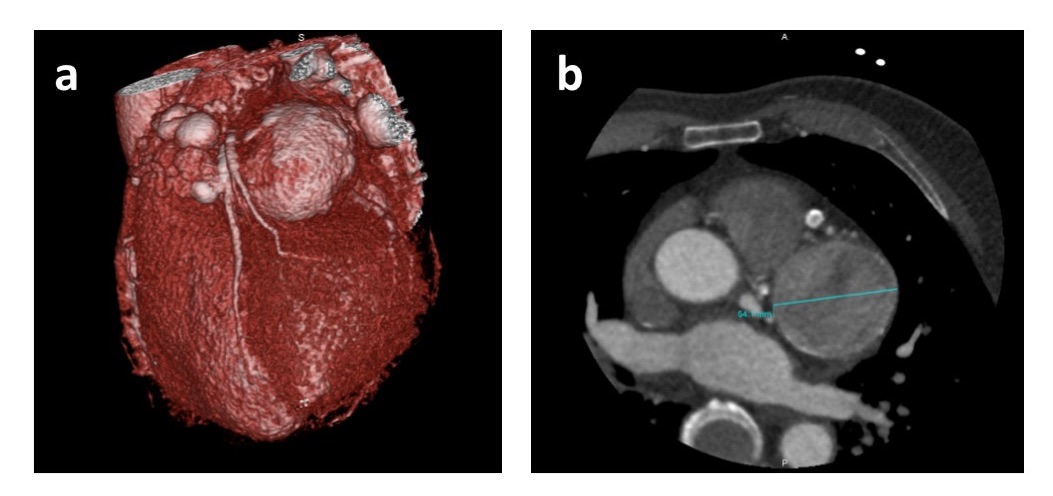
Figure 2: Imaging seven years later.
2a – Three-dimensional CT coronary angiogram image demonstrating enlargement of the main aneurysm to 51mm x 55mm.
2b – Axial image from CT coronary angiography demonstrating the aneurysm had increased in size to 51mm x 55mm. Low density is seen within the aneurysm suggesting either low flow or clot formation.
Discussion
Coronary artery fistulas (CAF) are anomalous terminations of the coronary arteries and are identified in 0.05% – 0.25% of patients who undergo coronary angiography.1 The majority of CAF are of congenital origin and adult patients are usually asymptomatic.1 Most CAF arise from the right coronary artery (50%), followed by the left coronary artery (42%) and less commonly both the right and left coronary arteries (5%).1 CAF involving the pulmonary trunk are very rare.
Vieussens’ arterial ring (VAR) is a collateral pathway between the conus branches of the right and left coronary arteries. It is a normal anatomical variant and is rarely associated with any pathological conditions. As was the case in this patient, the presence of both a CAF into the pulmonary trunk and an aneurysm within VAR is extremely rare with very few other reported cases.2 There is one report of rupture of a 3.5cm aneurysm of VAR that was successfully treated by surgical repair.3
The management of simple CAF is controversial. In asymptomatic patients there is no urgency to close CAF and close follow-up for several years is useful. Antiplatelet and prophylactic precautions against bacterial endocarditis are recommended.1 Surgical ligation and transcatheter embolization have similar early effectiveness and patients may have an excellent prognosis following either procedure.1 However, the optimum management for large and complex CAF (as in this case) is unknown. We would therefore welcome feedback from readers about how you feel this case could be managed.
Multiple Choice Questions
- Which coronary vessel do the majority of symptomatic CAF arise from?
- LCA
- RCA
- Circumflex
- LAD
- Both RCA and LCA
- What is the most common clinical presentation of CAF?
- Dyspnoea
- Chest pain
- Sudden death
- Continuous heart murmur
- Stroke
- What is the chance of spontaneous closure of a CAF?
- 0.01%
- 1%-2%
- 10 -15%
- 25%
- 50%
References
- Zenooz NA. et al. Coronary Artery Fistulas: CT findings. Radiographics 2009; 29:781-789.
- Lee HY, Cho SH. An Unusual Form of Coronary Artery Fistula: A Small Aneurysm of Vieussens’ Arterial Ring Communicating with the Pulmonary Artery. Korean J Thorac Cardiovasc Surg. 2014; 47:152-154
- Health A. Rupture of an aneurysm of Vieussens’ arterial ring presenting as acute cardiac tamponade. Clinical Radiology 2009; 64, 1129-1131
Answers1: 1 = b, 2 = d, 3 = b


