Will Loughborough, Stephen Lyen, Mark Hamilton
University Hospitals Bristol NHS Foundation Trust
A 30 year old woman with Tetralogy of Fallot was referred for a cardiac computed tomographic examination prior to cardiac surgery. She had a Tetralogy repair in childhood involving a transannular patch. She had developed severe pulmonary valve regurgitation and was undergoing work up for an open pulmonary valve replacement which included coronary arterial assessment. A cardiac MRI demonstrated restrictive RV physiology with early diastolic septal interaction and an end diastolic A wave in the main pulmonary artery flow curve. There was unexplained reduction in LV long axis shortening both on MRI and TTE with probably pseudonormal transmitral Doppler. A prospectively ECG gated coronary angiogram demonstrated unobstructed coronaries with normal origins. However, it revealed a thick slab of pericardial calcification extending along the posterior atrioventricular groove, with multiple prongs of calcification extending into the basal inferior and lateral left ventricular myocardium (see images) and a single prong into the RV myocardium.
On review, the extensive LV prongs corresponded to tethering of the left ventricle on dynamic imaging with consequent reduced long axis excursion. Both atria and their draining veins were dilated, implying elevated pressure (no shunt). The interatrial septum was central suggesting the pressure was equal. The right heart findings could be explained by the RV physiology. However, these do not explain the LA findings which would seem most elegantly explained by reduced LV filling, secondary to impaired LV long axis function with secondary diastolic dysfunction. At the same time, the pericardium compressed the LV diameter a little. The conclusion was that the RV dysfunction was substantially due to the pulmonary valve disease. However the LV anatomical and physiological parameters support a diagnosis of mild systolic and diastolic dysfunction. The calcified pericardium caused pericardial constriction leading to impaired ventricular filling. The prongs of calcified pericardium invading the LV myocardium caused restriction on long axis shortening and lengthening (leading to restrictive physiology).
The patient was discussed at the adult congenital cardiac MDT where the decision was to replace the pulmonary valve alone as extensive surgical debridement of the LV pericardium was not considered attractive.
Figure 1
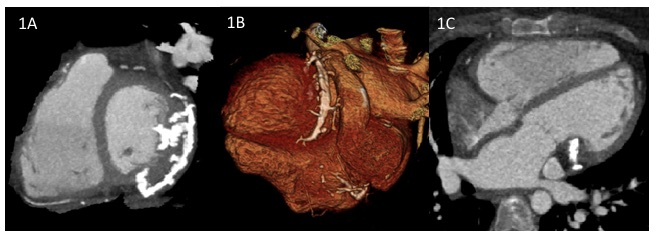
Figure legend
1A Short axis view. Multiple prongs of pericardial calcification extending into basal inferior and lateral left ventricular myocardium
1B Volume rendered image. Thick slab of pericardial calcification extending down the posterior atrioventricular groove
1C Four chamber long axis view. Pericardial calcification extending the basal left ventricular myocardium
Multiple choice questions
1. Treatment of Tetralogy of Fallot with a transannular patch is often associated with regurgitation though which valve?
- Tricuspid
- Pulmonary
- Mitral
- Aortic
2. Constrictive pathophysiology is usually due to abnormalities in the
- Myocardium
- Valves
- Coronaries
- Pericardium
3. Restrictive pathophysiology is usually primarily due to abnormalities in the
- Myocardium
- Pericardium
Answers
1 – B, 2 – D, 3 – A


