Author
Dr Ekene Kenneth Okonkwo1
1 Royal Liverpool University Hospital
Case history
67-year-old male patient presented with hypotension, abdominal pain and raised lactate levels. He had a background of previous stroke and left ventricular systolic dysfunction.
An urgent CT scan of the abdomen and pelvis in arterial and portal venous phases was done which showed a filling defect in the LV apex consistent with an apical thrombus. He also had an abdominal aortic aneurysm with mural thrombus and a proximally occluded superior mesenteric artery causing bowel ischaemia.
The patient had previously had a transthoracic echocardiogram a few months ago and was started on warfarin for the LV thrombus but this information was not communicated to the reporting radiologist at the time of the urgent CT abdomen and pelvis study.
This article highlights the importance of reviewing all available images of the heart on every CT of the abdomen and pelvis.
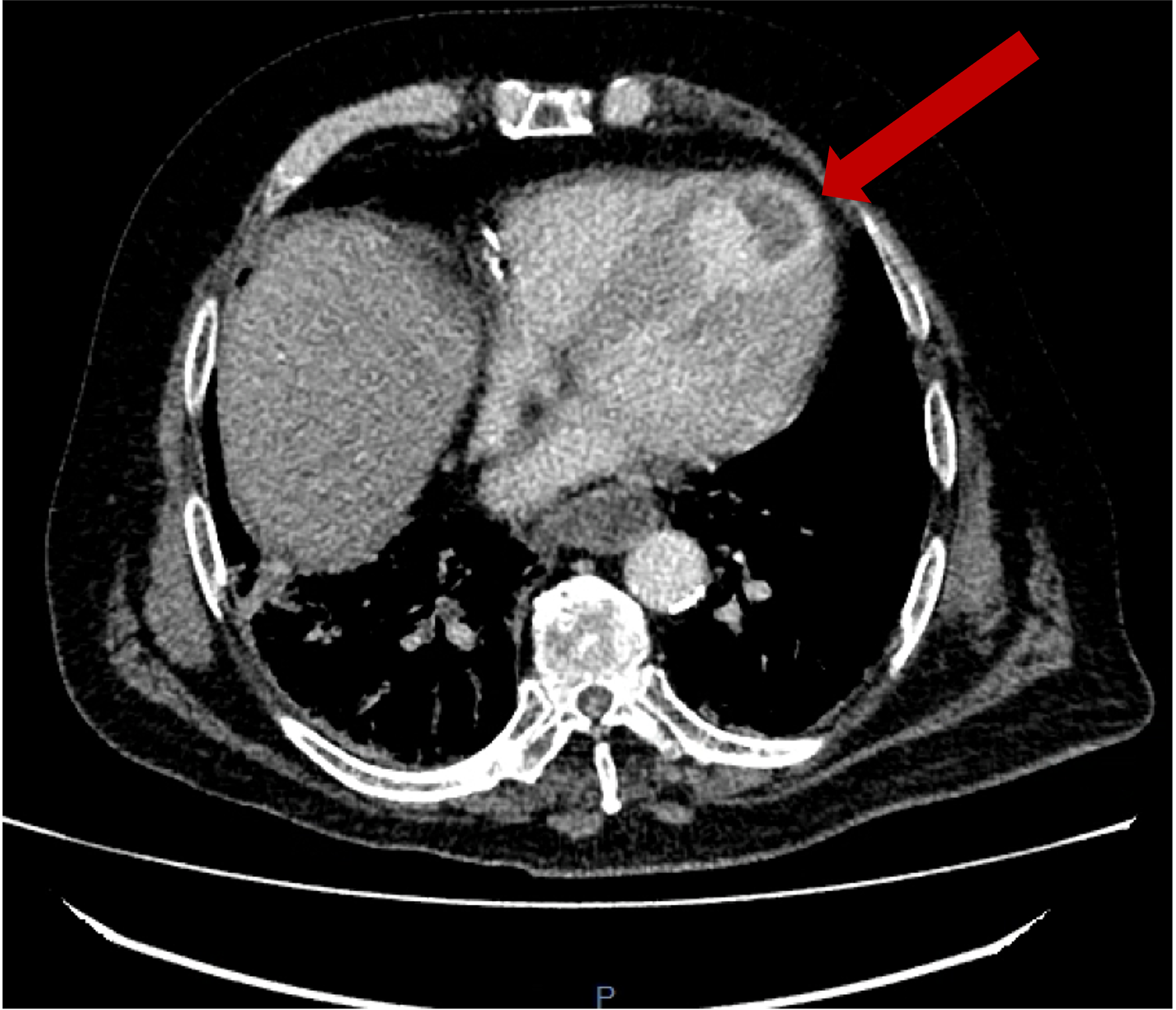
Arterial phase axial CT image of the lower chest showing a left ventricular apical thrombus.
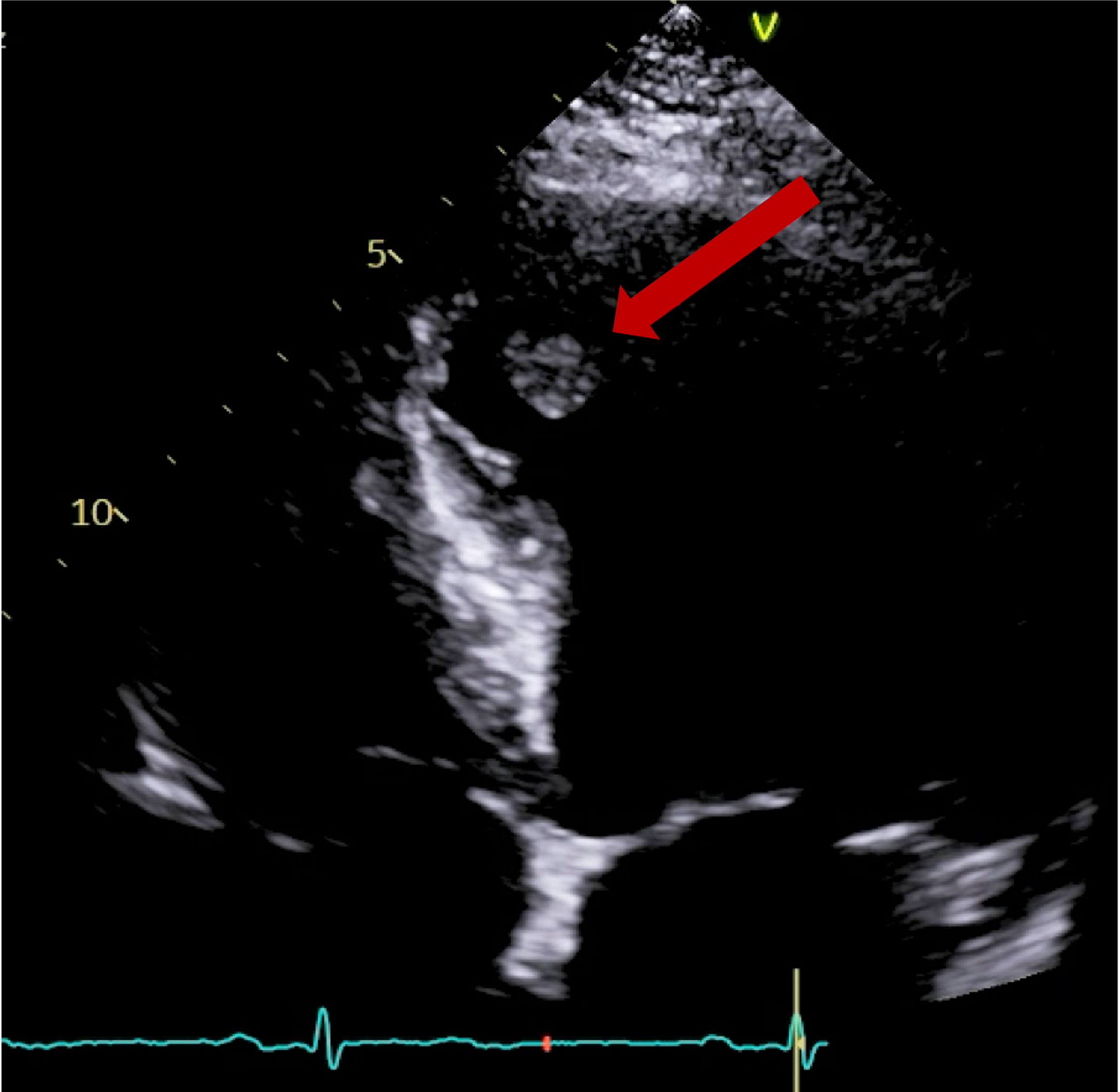
Transthoracic echocardiogram – apical 4-chamber view showing an apical thrombus in the left ventricle.
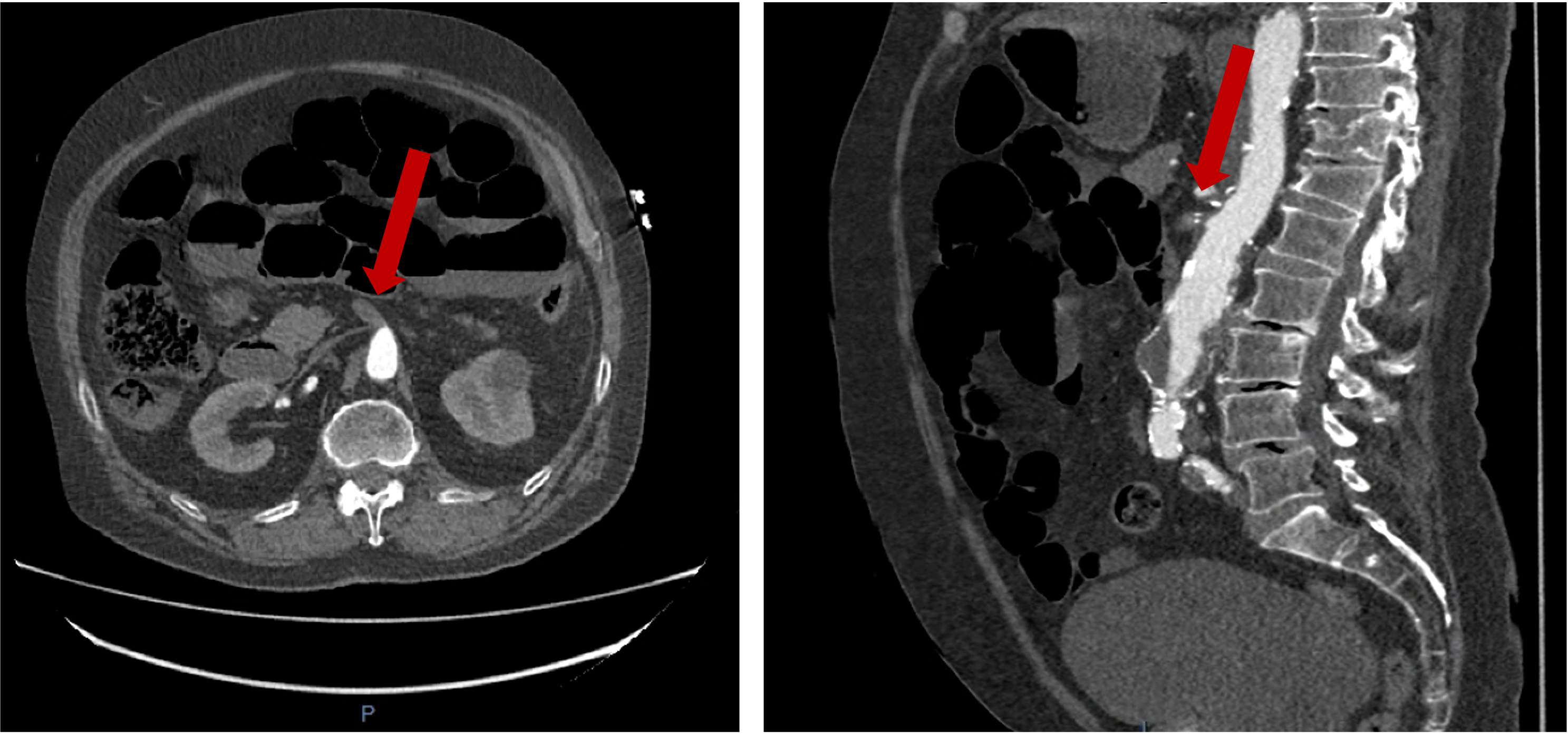
Arterial phase CT imaging of the abdomen showing thrombus in the proximal superior mesenteric artery on both axial and sagittal images.
Questions
Which one of the following statements is false?
- Severely impaired LV ejection fraction is a strong predictor of LVT formation after MI.
- Patients with dilated cardiomyopathy have a higher prevalence of thrombus than patients with ischaemic cardiomyopathy.
- Elevated D-dimer levels and reduced LV ejection fraction have been independently associated with an increased risk LV thrombus.
- Hypertrophic cardiomyopathy does not increase the risk of LV thrombus due to the increased myocardial LV wall thickness.
- LV thrombus is mostly diagnosed incidentally on transthoracic echocardiography.
Which statement is most accurate?
- Pedunculated LV thrombi are at greater risk of embolic phenomenon compared with mural thrombus.
- Transoesophageal echocardiography is particularly useful in detecting LV thrombus.
- Contrast enhanced transthoracic echocardiography has no role in detection of LV thrombi.
- Contrast enhanced cardiac CT should never be used in detection of left sided cardiac thrombus because of high radiation dose.
- Tissue characterisation of left sided cardiac thrombi is excellent with contrast enhanced cardiac CT.
Regarding the role of CMR (cardiac magnetic resonance) in detecting LV thrombus, which one the following statements is false?
- CMR is considered the best imaging technique for detection of LV thrombus.
- CMR is great for tissue characterisation.
- CMR has high spatial and temporal resolution as well as high soft tissue contrast.
- CMR is particularly helpful in acutely unwell patients who cannot undergo transthoracic echocardiography.
- CMR can also assess cardiac function, valvular anatomy, and perfusion.
(Answers:d,a,d)
Reference:
1. Catalani, Filippo, et al. “Left Ventricular Thrombosis in Ischemic and Non-Ischemic Cardiomyopathies: Focus on Evidence-Based Treatment.” Journal of Clinical Medicine5 (2025): 1615.


