The elusive napkin ring sign
Authors and affiliations
- Sai Viswan Thiagarajah, Medical Student, University of Edinburgh
- Michelle C Williams, Consultant Radiologist, Centre for Cardiovascular Science, University of Edinburgh, Edinburgh, UK
Case history
A 58-yr old female presented to the emergency department with heavy central chest pain. It was relieved with sublingual glyceryl trinitrate(GTN) and resolved by the time she arrived at the hospital.
She had a previous history of coronary artery disease and suffered a non-ST elevation myocardial infarction (NSTEMI) 1 year previously. An invasive coronary angiogram performed at this time showed severe stenosis in the distal right coronary artery, which was treated with a stent. She had a history of hypertension and a family history of coronary artery disease. She was an ex-smoker with a significant pack year history.
An electrocardiogram (ECG) showed longstanding T wave inversion, but was otherwise unremarkable. High sensitivity troponin on admission was 5 ng/L, and a repeat at 3 hours later was 4 ng/L. She was discharged and followed up with an outpatient computed tomography coronary angiogram (CTCA) which is shown below.
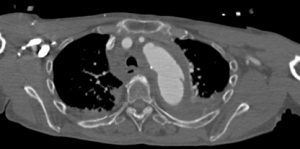
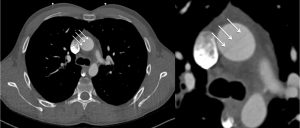
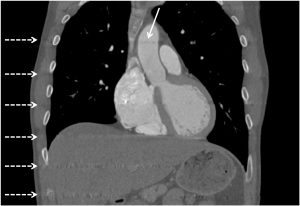
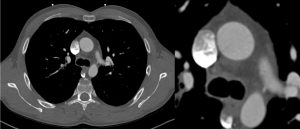
Image
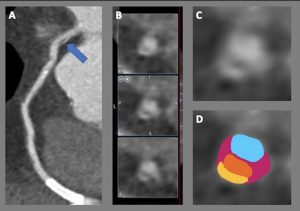
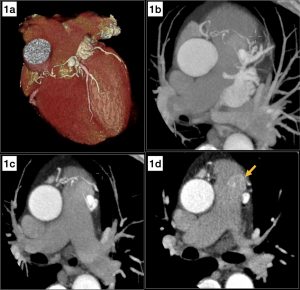
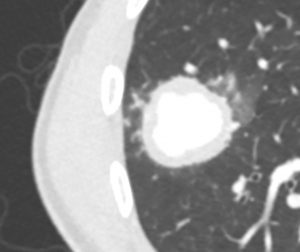
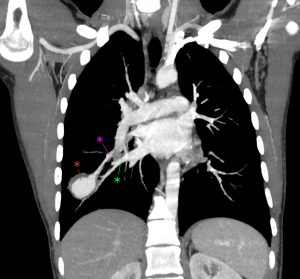
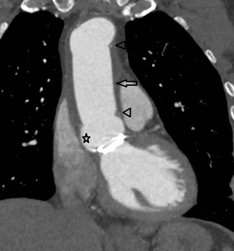
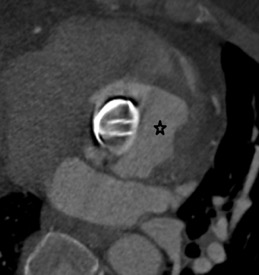
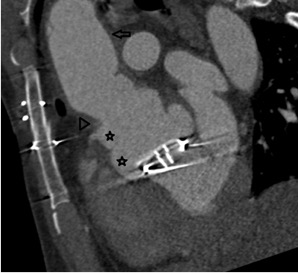
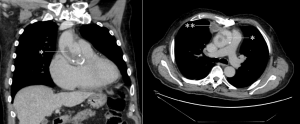
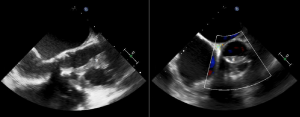
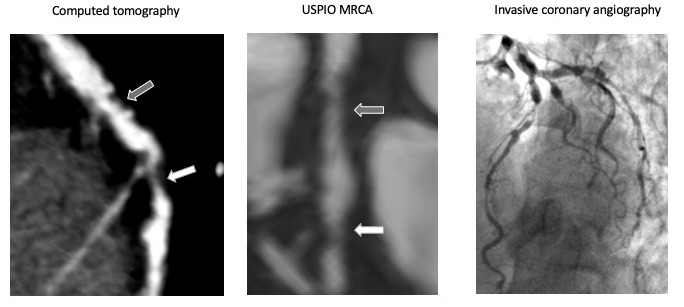
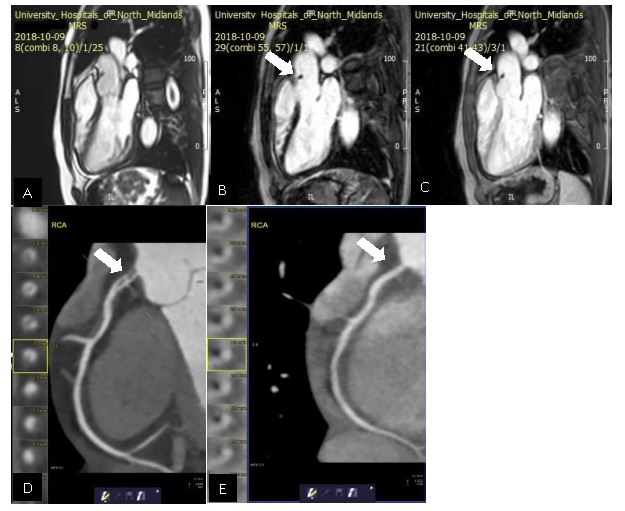
CTCA identified a napkin ring sign in the proximal right coronary artery. Image (A) shows a curved planar reformation of the right coronary artery with an arrow showing the area of the napkin ring sign in the proximal vessel and a patent stent in the distal vessel. (B) shows cross sectional images through the proximal right coronary artery showing three images of the napkin ring sign at 1 mm intervals along the vessel lumen. (C) shows a zoomed in cross sectional image of the napkin ring with (D) showing corresponding labelled components.
Questions & best answers
- Which of the following are described as ‘high risk’ features for a plaque seen on CT coronary angiography
-
- Napkin ring sign
- Positive vessel remodelling
- Spotty calcification
- Low attenuation
- All of the above
2. Which of the following correctly describes the napkin ring sign?
-
- Calcified plaque with positive vessel remodelling, low attenuation centre and high attenuation peripheral rim
- Non-calcified plaque with positive vessel remodelling, low attenuation centre and a high attenuation peripheral rim
- Calcified plaque with positive vessel remodelling, high attenuation centre and low attenuation peripherally
- Non-calcified plaque with positive vessel remodelling, high attenuation centre and low attenuation peripherally
- Calcified plaque with positive remodelling, low attenuation centre, and an isointense peripheral rim.
3. Which of the following is the denotation used in the CAD RADS (Coronary Artery Disease Reporting and Data System) when an adverse plaque feature is seen
-
- CAD RADS 4
- CAD RADS 5
- Modifier V
- Modifier G
- Modifier S
Answers
- E – all of these have been described as high risk/adverse plaque features
- B – In the D shown above, blue represents the lumen, orange represents the low attenuation centre of the napkin ring, pink represents non calcified plaque and yellow represents the high attenuation rim
- C – CAD RADS 4 and 5 describe the degree of vessel stenosis, modifier G is for grafts, S is for stents and V is for vulnerable/adverse plaque features
Discussion
CTCA can identify features of high-risk plaques (also called vulnerable plaques, or adverse plaque characteristics) that are thought to be associated with the thin cap fibroatheroma, the histological precursor of ruptured plaques.
Positive vessel remodelling refers to a plaque with the outer vessel diameter > 1.1 times that of the adjacent uninvolved vessel(1). A low attenuation plaque is a non-calcified plaque measuring < 30 Hounsfield units. Spotty calcifications are small, calcified plaques < 3mm in diameter in any direction(2). The napkin ring sign refers to a combination of plaque characteristics where there is a non-calcified plaque with positive remodelling, a low attenuation plaque centre and a higher attenuation peripheral rim, as seen in this case(3). Reporting of these features is recommended in the Coronary Artery Disease Reporting and Data System (CAD RADS), but observer agreement amongst expert readers is only ‘fair’(4).
Several studies have evaluated the usefulness of these vulnerable plaque characteristics for assessing risk of clinical outcomes. Motoyama et al. showed that, those with adverse plaque features were ten times more likely to develop an acute coronary syndrome at 4 year follow up(5). In the PROMISE trial, adverse plaque features was associated with an increased risk of MACE (major adverse cardiovascular events), particularly amongst women and younger patients(6). In the SCOT-HEART trial, adverse plaque characteristics were associated with an increased risk of fatal or non-fatal myocardial infarction, with the greatest risk seen in those with adverse plaques and obstructive coronary artery disease(7). However, in the SCOT-HEART trial adverse plaque characteristics were not an independent predictor of outcomes when controlled for coronary plaque burden assessed with calcium score.
The napkin ring sign has been shown to be a particularly high-risk plaque feature. Maurovich-Horvat et al. showed that the napkin ring sign was associated with histologically advanced atherosclerotic lesions (per plaque sensitivity 36%, specificity 100%)(8). In another study it was also found to be a predictor of subsequent acute coronary syndrome 3 years after follow-up(9). Puchner et al. studied 472 patients with chest pain suspicious of ACS who underwent CTCA(2). The incidence of a napkin ring sign was around ten times greater in those found to have ACS than those without (32.4% vs 3.2%).
However, the napkin ring sign is not a particularly common finding on CTCA. In the SCOT-HEART trial the napkin ring occurred in 0.3% (78 of 26,525) of vessel segments analysed(7). Otsuka et al identified it in 0.4% (45 of 12,727) of segments(9). Uncertainty also remains as to what exactly the napkin ring sign represents – is it focal ulceration, contrast enhancement with the vasovasorum, low density calcification, or something else? The management of these CTCA findings is also uncertain. There are no randomised controlled trials assessing the impact of different management strategies on the progression of these plaques, or subsequent clinical outcomes.
Learning points
- Adverse plaque features are common on CTCA but inter-observer ability to recognise their presence is variable
- The napkin ring sign is the least common of the adverse plaque features but potentially the most clinically significant
- More research is required to understand whether patients with these adverse plaque features on CTCA would benefit from more aggressive management
References
-
Pundziute G, Schuijf JD, Jukema JW, Decramer I, Sarno G, Vanhoenacker PK, et al. Evaluation of plaque characteristics in acute coronary syndromes: Non-invasive assessment with multi-slice computed tomography and invasive evaluation with intravascular ultrasound radiofrequency data analysis. Eur Heart J [Internet]. 2008 Oct [cited 2021 May 5];29(19):2373–81. Available from: https://pubmed.ncbi.nlm.nih.gov/18682447/
-
Puchner SB, Liu T, Mayrhofer T, Truong QA, Lee H, Fleg JL, et al. High-risk plaque detected on coronary CT angiography predicts acute coronary syndromes independent of significant stenosis in acute chest pain: Results from the ROMICAT-II trial. J Am Coll Cardiol. 2014 Aug 19;64(7):684–92.
-
Vulnerable plaque | Radiology Reference Article | Radiopaedia.org [Internet]. [cited 2021 May 17]. Available from: https://radiopaedia.org/articles/vulnerable-plaque?lang=gb
-
Maroules CD, Hamilton-Craig C, Branch K, Lee J, Cury RC, Maurovich-Horvat P, et al. Coronary artery disease reporting and data system (CAD-RADSTM): Inter-observer agreement for assessment categories and modifiers. J Cardiovasc Comput Tomogr. 2018 Mar 1;12(2):125–30.
-
Motoyama S, Ito H, Sarai M, Kondo T, Kawai H, Nagahara Y, et al. Plaque characterization by coronary computed tomography angiography and the likelihood of acute coronary events in mid-term follow-up. J Am Coll Cardiol. 2015 Jul 28;66(4):337–46.
-
Ferencik M, Mayrhofer T, Bittner DO, Emami H, Puchner SB, Lu MT, et al. Use of high-risk coronary atherosclerotic plaque detection for risk stratification of patients with stable chest pain: A secondary analysis of the promise randomized clinical trial. JAMA Cardiol [Internet]. 2018 Feb 1 [cited 2021 Jun 10];3(2):144–52. Available from: https://pubmed.ncbi.nlm.nih.gov/29322167/
-
Williams MC, Moss AJ, Dweck M, Adamson PD, Alam S, Hunter A, et al. Coronary Artery Plaque Characteristics Associated With Adverse Outcomes in the SCOT-HEART Study. J Am Coll Cardiol [Internet]. 2019 Jan 29 [cited 2021 May 17];73(3):291–301. Available from: /pmc/articles/PMC6342893/
-
Maurovich-Horvat P, Schlett CL, Alkadhi H, Nakano M, Otsuka F, Stolzmann P, et al. The napkin-ring sign indicates advanced atherosclerotic lesions in coronary CT angiography. JACC Cardiovasc Imaging. 2012 Dec 1;5(12):1243–52.
-
Otsuka K, Fukuda S, Tanaka A, Nakanishi K, Taguchi H, Yoshikawa J, et al. Napkin-ring sign on coronary CT angiography for the prediction of acute coronary syndrome. JACC Cardiovasc Imaging. 2013 Apr;6(4):448–57.
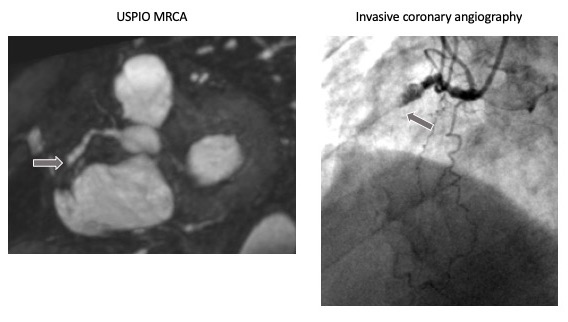
 Image 3- Nodal artery arising from LCX
Image 3- Nodal artery arising from LCX